


Sternotomy vs Thoracotomy for Coarctation with Arch Hypoplasia: Prioritizing Adequate Transverse Arch Size to Optimize Long-term Arch Repair Outcomes Given Clinically Insignificant Recovery Differences
*Dominic Recco MD, *Shannen Kizilski , *Kimberlee Gauvreau , *Breanna Piekarski , *Ashwin Prakash , *David Hoganson
Cardiac Surgery, Boston Children's Hospital, Boston, MA
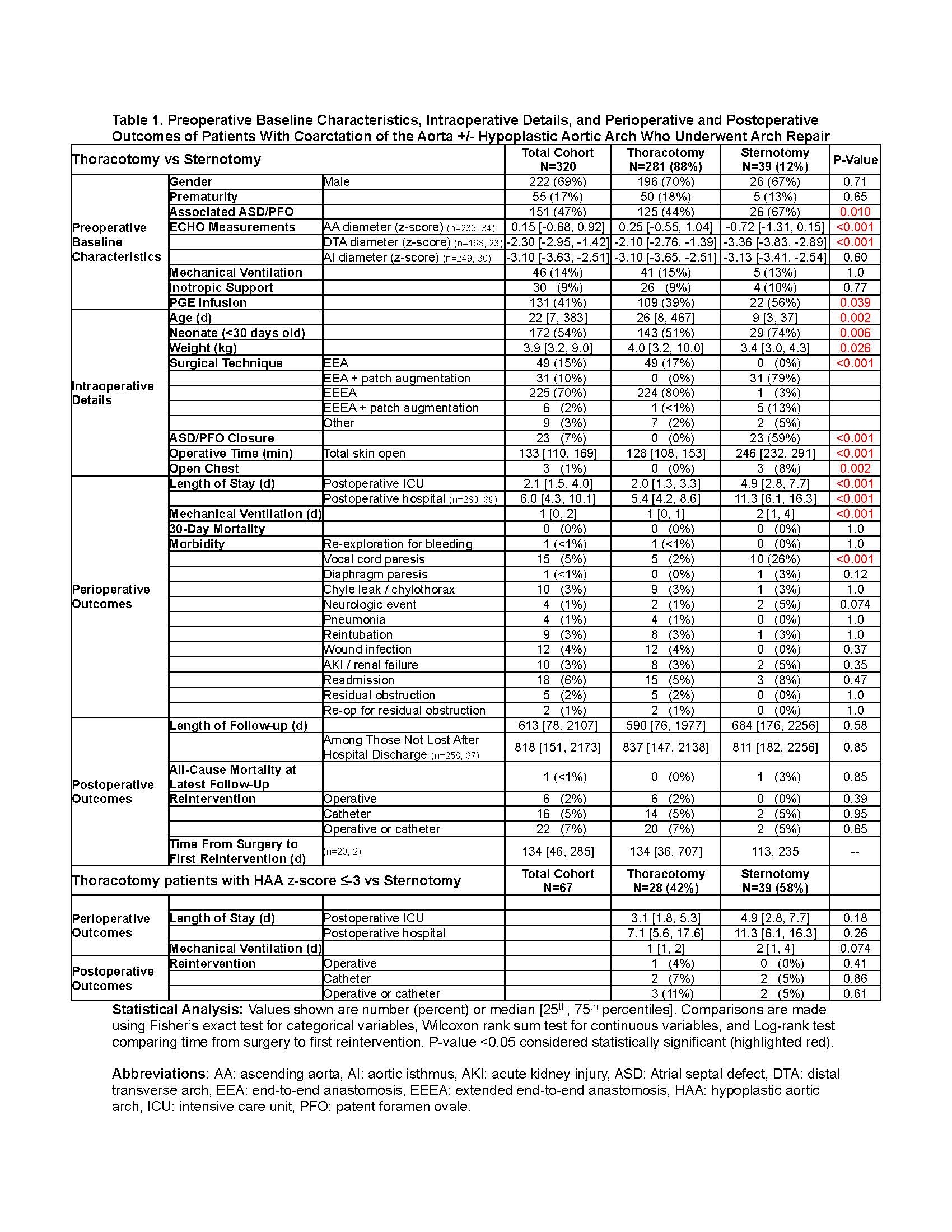
Background: Residual transverse arch hypoplasia after coarctation (CoA) repair in childhood is associated with early MI and stroke in adulthood. The threshold for acceptable mild transverse arch hypoplasia is under investigation, and it is expected that a more aggressive approach to address hypoplastic aortic arch (HAA) via sternotomy with patch augmentation is warranted to reduce the long-term risk of elevated resistance across the arch and subsequent impact on the coronary and cerebral circulation. This study investigated the difference in hospital course and outcomes between CoA repair via thoracotomy or via sternotomy. Study Design: Patients with CoA +/- HAA who underwent CoA repair at our institution from 2012 to 2022 were reviewed with exclusion of significant concomitant procedures including VSD closure. Repair was performed via sternotomy (n=39) or thoracotomy (n=281, with 70% having extended end-to-end anastomoses). Results: Sternotomy patients had longer ventilation duration (2[1,4] vs. 1[0,1]d) and ICU (4.9[2.8,7.7] vs. 2.0[1.3,3.3]d) and hospital (11.3[6.1,16.3] vs. 5.4[4.2,8.6]d) lengths of stay (LOS) (p<0.001 each). Stratifying thoracotomy patients by HAA z-score ?-3, there were no differences in ventilation duration, ICU LOS or hospital LOS between sternotomy and thoracotomy patients. Operative and latest follow-up mortality were not different between the sternotomy and thoracotomy groups (p=1.0 and p=0.85, respectively). Freedom from catheter-based or operative reintervention at 10y was 93% for sternotomy vs. 83% for thoracotomy. Complications including diaphragm paresis, chylothorax, neurologic events, and readmission were not different between the two groups. Conclusions: Repair of CoA with HAA via sternotomy vs. thoracotomy has numerically different but clinically insignificantly longer ventilator duration, ICU LOS and hospital LOS, given the devastating potential long-term consequences of early MI and stroke with residual arch hypoplasia. Furthermore, these differences were eliminated if the transverse arch was z-score ?-3. There is no mortality difference between groups with a trend toward lower reintervention in the sternotomy group. Further work is required to define the threshold for patch augmentation of transverse arch hypoplasia to avoid long-term risk, but that threshold should focus on optimizing long-term outcomes given that recovery differences between sternotomy and thoracotomy are clinically insignificant.
Back to 2024 Abstracts