


Disparities in Opioid Prescribing in Traumatically Injured Patients
*Sophia M. Smith 1, *Rachel Adams PA-C1, *Emily J. Ha BS2, *Cara Michael BA2, *Kendall Jenkins MS2, *Wang Pong Chan BS2, *Noelle N. Saillant MD1, *Jeffrey Franks MSPH1, *Sabrina Sanchez 1
1Boston Medical Center, Quincy, MA; 2Boston University Chobanian & Avedisian School of Medicine, Boston, MA
Objective Disparities in opioid prescribing are well-documented, albeit not in the trauma population, where disadvantaged communities are overrepresented. We sought to evaluate disparities in opioid administration trends after traumatic injury.
Design Single-institution retrospective cohort study.
Setting Urban, safety net, level 1 trauma center.
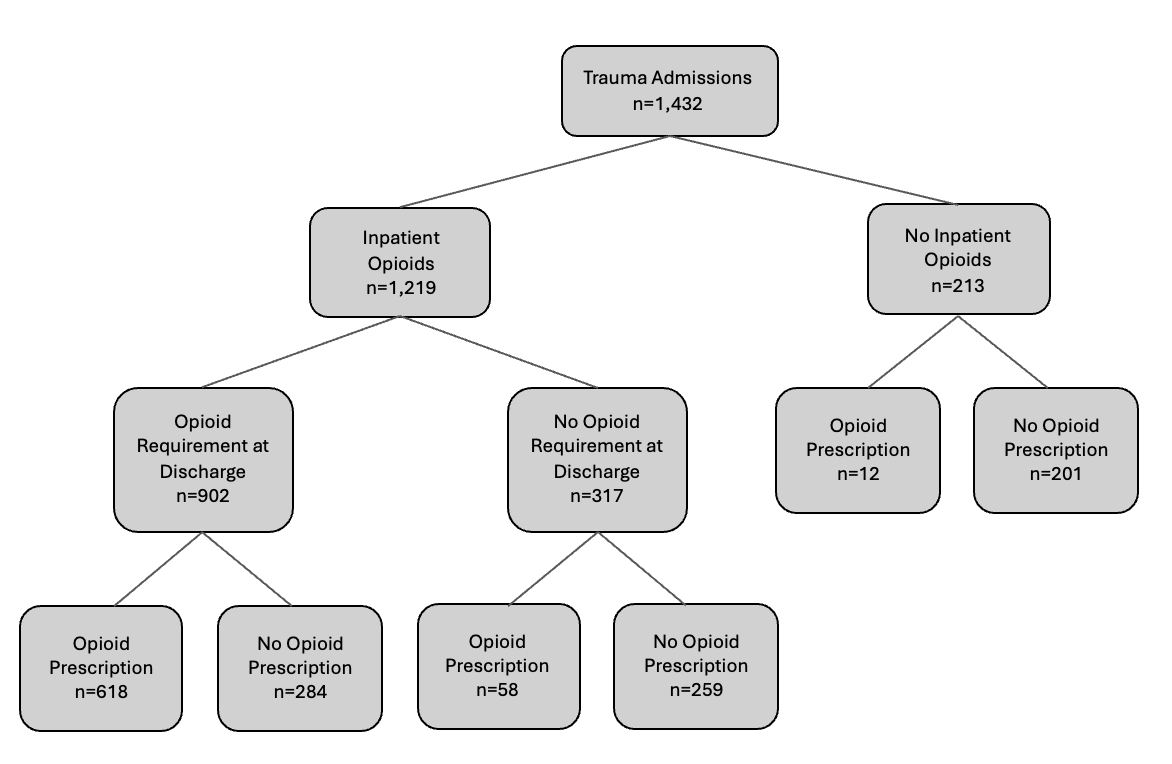
Patients All adult trauma admissions over a four-year time period, 2018-2021. The total study cohort included 1,432 traumatically injured patients.
Main Outcome Measures The primary outcomes were mean daily opioid requirement during hospitalization and the day prior to discharge, opioid receipt at discharge, and number of day of pain control prescribed at discharge. Opioids were quantified in milligram morphine equivalents (MME). Pain control days prescribed at discharge were calculated based on MMEs administered within the 24-hour period prior to discharge.
Results Of 1,432 patients, 902 (63%) required opioids 24 hours prior to discharge; only 618 of these (69%) were discharged with opioids. Higher hospitalization MMEs were associated with homelessness (b 29.21, p=0.03), depression/anxiety (b 29.28, p=0.003), and substance use disorder (SUD) (b 48.76, p<0.001); non-white patients had lower hospitalization MMEs (b -20.3, p=0.03). Among patients requiring opioids on discharge, those with SUD had lower odds of discharge opioid prescriptions (OR 0.64, 95% CI 0.42-0.97, p=0.03). A negative correlation was observed between MME requirement at discharge and prescribed pain control days (IRR 0.998, 95% CI 0.997-0.999, p<0.001).
Conclusions Sociodemographic disparities in opioid prescribing persist in trauma patients, with racial disparities in dosing and lower odds of discharge opioid prescriptions in patients with SUD despite higher inpatient needs. The inverse association between MME requirements and prescribed pain control days highlights the need for careful evaluation of discharge pain management practices.
Back to 2024 Abstracts