


Heart Transplant Equity: The Effects of the 2018 Allocation Policy Change on White and Black/Hispanic Recipient Mortality and Morbidity
*Alisa Pugacheva 1, *Selena Li MD1, *Asishana Osho MD, MPH1, *Thais Faggion Vinholo MD, MSc2, *Eriberto Michel MD1, *Thoralf M. Sundt MD1
1Division of Cardiac Surgery, Massachusetts General Hospital, Boston, MA; 2Division of Cardiac Surgery, Brigham and Women's Hospital, Boston, MA
Objective:We aim to assess differences in mortality and posttransplant outcomes in White(W) compared to Black and Hispanic(B/H) patients before and after the 2018 policy change.
Design:Cohort study(1/1/2014-12/31/2021) from the UNOS heart transplant database.
Setting:Public and private transplant centers.
Patients:9,155 patients included.Loss to follow-up, multiorgan, <6 months post-transplant and prior heart transplants were excluded.Propensity-matching and subgroup analysis were performed to evaluate factors associated with posttransplant outcomes pre- and post-policy change; matching factors:payment type, recipient employment, days and status on waitlist, recipient citizenship, donor and recipient ethnicity, UNOS region, recipient education, distance to transplant center, ventilation, transfusion, high creatinine, inotropes, ventricular assistance device(VAD), ejection fraction, ischemic time, extracorporeal membrane oxygenation(ECMO), intra-aortic balloon pump(IABP) and donor comorbidities(diabetes, hypertension, high-risk status).
Intervention:The 2018 heart transplant policy change(10/18/2018), an expansion of the 3-tier to a 6-tier acuity system, meant to reduce waitlist mortality and improve transplant rates to more medically urgent cases.
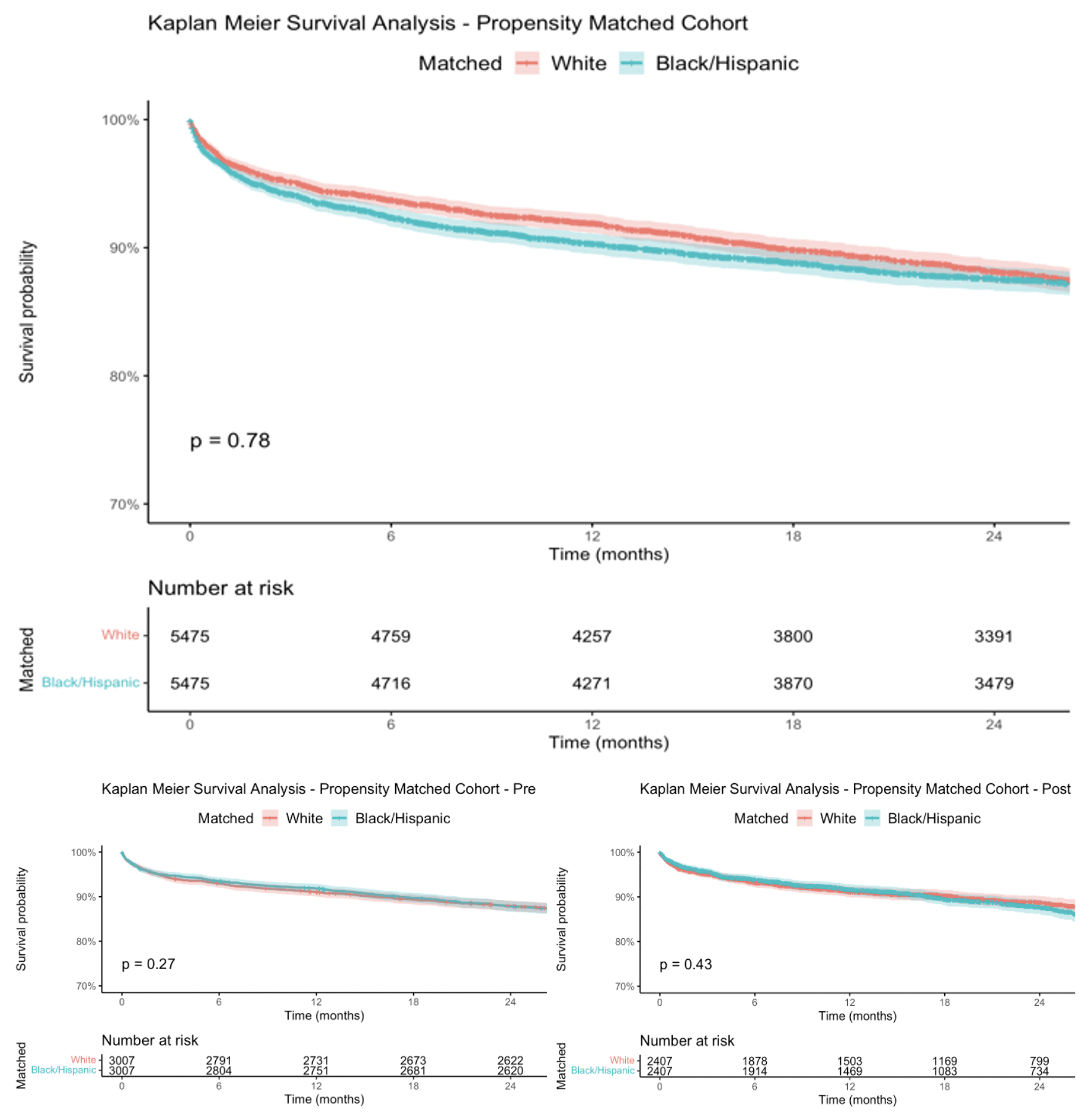
Results:W recipients had primarily W donors compared to B/H recipients(67.5% vs. 58.4%,p<0.001), and B/H recipients, B/H donors compared to W recipients(30.1% vs. 39%,p<0.001) in both periods. Unmatched outcomes showed B/H recipients had more acute rejection episodes than W recipients’ pre-allocation(23.8% vs 20.2%,p<0.001), but no significant difference post-allocation.B/H patients received more treatment for rejection 1 year from transplant in both periods (pre:19.4%vs.16.7%,p=0.001, post:16.1% vs. 13.9%,p=0.007).After propensity matching, these differences were not statistically significant.Matched Kaplan-Meyer survival curves showed no significant difference between overall survival of W vs B/H recipients(p=0.78).B/H ethnicity was not a significant risk factor for overall mortality on univariable and multivariable Cox regression.Examining mortality risk factors showed Private Insurance was protective in W recipients(HR=0.85,95%CI:(0.77,0.94),p=0.001), and ventilation was harmful(HR=2.21,(1.57,3.11),p<0.001).For B/H recipients, non-citizen status(HR=0.72,(0.54,0.96),p=0.025), Private insurance(HR=0.82,(0.72,0.94),p=0.005), and higher educational attainment(HR=0.75,(0.58,0.95),p=0.018) were protective, and diabetes(HR=1.16,(1.02,1.32),p=0.027) was harmful.
Conclusion:While initial disparities in acute rejection were seen between W and B/H cohorts, they resolved after propensity matching.No significant differences were seen in overall survival between W and B/H recipients, but subgroup analyses revealed nuanced risk factors, such as citizenship, insurance, and payment type, emphasizing the need for comprehensive considerations in transplant policy and clinical decision-making to ensure equitable outcomes.
Back to 2024 Abstracts