Back to 2025 Abstracts
Sex Based Differences in Outcomes Following Thymectomy for Myasthenia Gravis
Carly Thaxton
*, Zane J. Hellmann, Daniel G. Solomon, Emily R. Christison-Lagay
Surgery, Yale School of Medicine, New Haven, CT
Introduction:
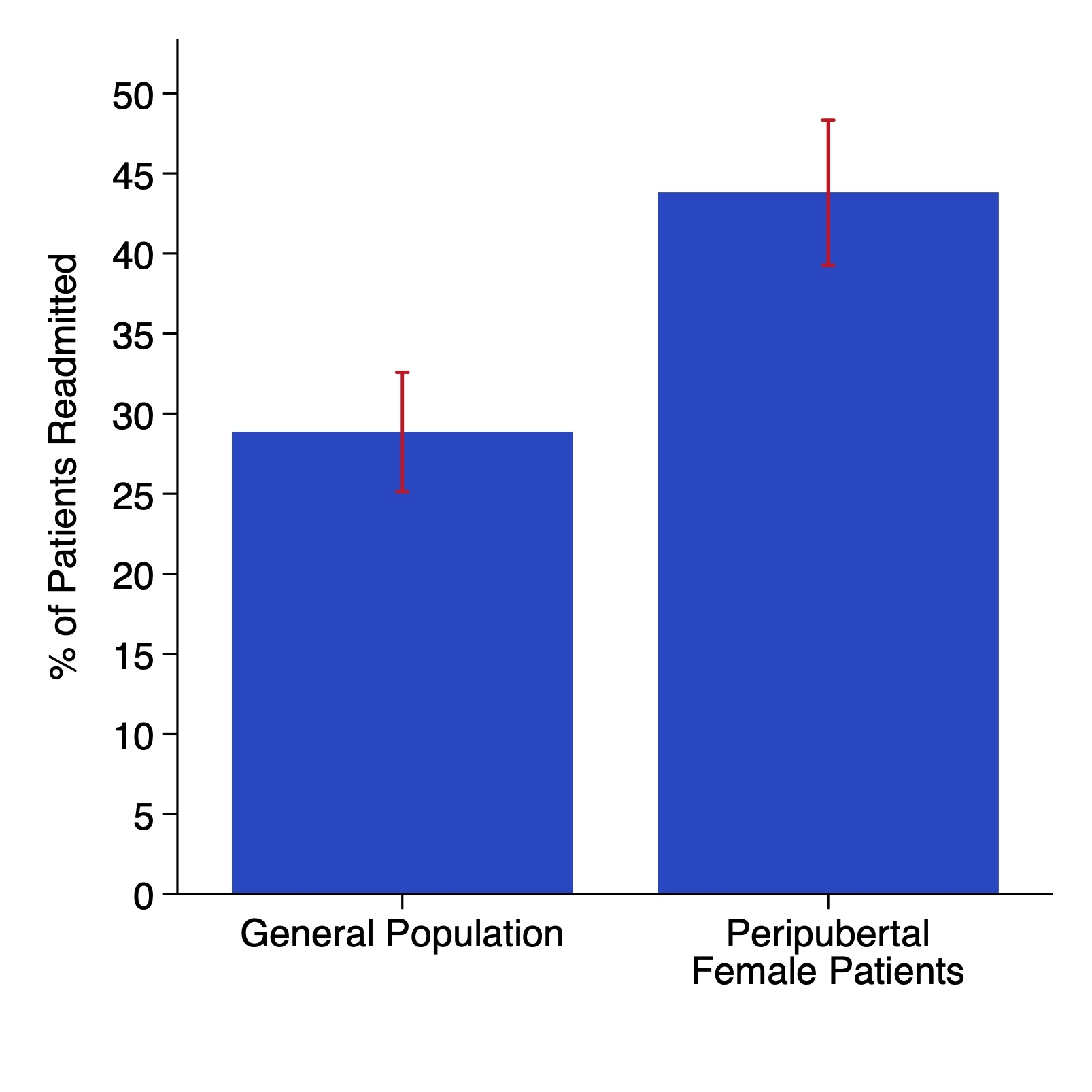
Previous literature has suggested that peripubertal female patients exhibit a more severe form of juvenile myasthenia gravis, as compared to male and prepubertal female patients. It was hypothesized that female patients 12 years or older at time of primary thymectomy would be significantly more likely to require readmission for respiratory illness or distress following thymectomy when compared to other pediatric patients.
Methods:
The Pediatric Health Information System (PHIS) database was queried for all patients 18 years old or younger who underwent thymectomy for myasthenia gravis between 2016-2023. Patients were followed until end of 2024 for all subsequent readmissions. Primary outcome was all readmissions with a diagnostic code associated with respiratory illness or respiratory distress, with secondary outcomes including any readmission during which a patient was mechanically ventilated.
Results:
There were 270 patients who required thymectomy for myasthenia gravis. A majority of patients were female (70.0%), non-white (68.2%), and 12 years or older (63.0%) at time of primary thymectomy. There were 121 peripubertal female patients (44.8%), who were both female and 12 years old older at time of primary repair. Following primary thymectomy, 98 (35.4%) patients had a readmission with a diagnostic code related to respiratory illness/distress, and 14 patients (5.1%) had a readmission during which they were mechanically ventilated. Female patients were significantly more likely to require readmission compared to male patients (39.7% vs 25.9%, p=0.03). There was a trend towards increased readmission rates among patients 12 years or older as compared to those less than 12 years of age at time of primary thymectomy (39.4% vs 29.0%, p=0.08). Peripubertal female patients were significantly more likely to require readmission, when compared to the general population (43.8% vs 28.9%, p=0.01). There was a trend towards higher readmission rates in peripubertal female patients, when compared to prepubertal female patients (43.8% vs 32.4%, p=0.12). There was no significant difference in likelihood of subsequent mechanical ventilation when comparing peripubertal female patients and the general population (5.8% vs 4.0%, p=0.50). Multivariable logistic regression demonstrated that female sex (OR 1.82, 95% CI 1.02-3.25, p=0.04) was significantly associated with subsequent readmission, with a trend towards increased likelihood of readmission for each additional year in age at time of primary thymectomy (OR 1.06, 95% CI 0.999-1.13, p=0.052).
Conclusion:
There is a paucity of data regarding post-thymectomy outcomes in the pediatric population. These data demonstrate that there are significant differences in outcomes for peripubertal female patients when compared to the general population. There is a need for further investigation into this subpopulation of patients to better characterize what may be leading to these worse outcomes.
Table 1
| | Male and Prepubertal Female Patients
(n = 149) | Peripubertal Female Patients
(n = 121) | p-value |
| White (%) | 44 (29.5%) | 42 (34.7%) | 0.36 |
| Commercial Insurance (%) | 64 (43.0%) | 63 (52.1%) | 0.14 |
| Admit Age In Years, Median (IQR) | 10 (6, 13) | 15 (13, 16) | <0.001 |
| Readmission for Respiratory Illness | 43 (28.9%) | 53 (43.8%) | 0.011 |
| Mechanical Ventilation | 6 (4.0%) | 7 (5.8%) | 0.50 |