Back to 2025 Abstracts
Survival after Pathologic Complete Response in Pancreatic Adenocarcinoma
Anays Murillo
*, Sing Chau Ng, Sara Myers, Kelly Kenzik, Teviah E. Sachs
Boston Medical Center, Brookline, MA
Background. Multimodal therapy has become a central approach in the treatment of pancreatic ductal adenocarcinoma (PDAC). With the increased utilization of neoadjuvant therapy (NT) we have seen a growing, albeit small population of patients achieving a pathologic complete response (pCR) following NT and surgical resection. We sought to better understand this patient population to see what characteristics might play a role in long term survival.
Study Design. The National Cancer Database was queried for patients diagnosed with PDAC who experienced a pCR (pT0 and pN0) following NT and pancreatectomy (2004-2021). NT was defined as either chemoradiation or chemotherapy alone. Duration of NT was defined as the time between the start of treatment and the day of surgery. Patients were categorized into groups based on length of survival. We explored two separate time points: 3 years and 5 years. Due to limited numbers within the cohort, we could not analyze shorter intervals. Chi-square analysis was used to compare demographic and clinical variables. Multivariable logistic regression was used to identify predictors for 3- and 5-year survival time points. P<0.05 was significant.
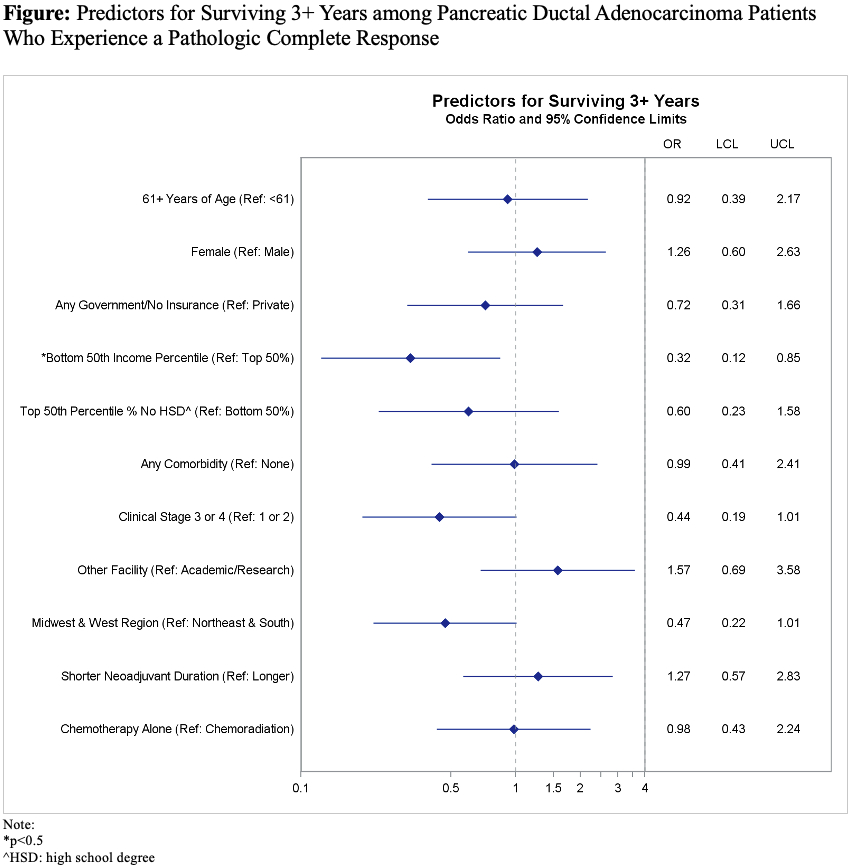
Results.There were 163 patients in the cohort. Median age was 61 years. About half (53%) of patients were male. Median duration of NT was 167 days. Most patients (87%) had multiagent chemotherapy. Almost two-thirds (65%) of the cohort received radiation in addition to chemotherapy as part of their NT and 21% also received adjuvant therapy. Many patients (73%) survived 3 years or more and slightly over half (56%) of patients survived 5 years or more. Age, sex, insurance status, education, comorbidity, facility type/region, duration of NT, and addition of radiation to NT did not predict surviving 3+ years vs <3 years. While clinical stage was significant in univariate analysis (p=0.04), it was not significant in multivariable modeling. Income in the lower two quartiles decreased the odds of surviving 3+ years (OR 0.32, 95% CI: 0.12-0.85, p=0.02). Comparing demographic and clinical variables using the survival points <5 years and 5+ years did not result in any significant associations.
Conclusion. Our data suggest no strong evidence for specific demographic, perioperative or tumor specific characteristics that are associated with better or worse overall survival in PDAC patients who achieve a pCR after NT and surgical resection. Although our sample size is small, it is sourced from a large national database, adding value to our findings. Interestingly, even the clinical stage of the tumor did not appear to have an impact on overall survival.