Back to 2025 Abstracts
Emergency Conversion to Open-Heart Surgery After TAVR: High Mortality and Steady Conversion Rates
Girinandan Konireddy
*, Salman Zaheer, Sari Holmes, Hamza Aziz, Matthew Czarny, Faisal Rahman, Rani Hasan, James Gammie, Michael Robich
Cardiac Surgery, Johns Hopkins University, Winter Garden, FL
Background: Catastrophic intra-procedural complications requiring emergency open-heart surgery (EOHS) during transcatheter aortic valve replacement (TAVR) are uncommon but poorly characterized. We aimed to determine the incidence, risk profile, procedural subtypes, outcomes, and factors associated with EOHS in a national TAVR cohort.
Methods: We identified all TAVR admissions from 2016�2020 in the Nationwide Inpatient Sample (NIS). EOHS patients were compared to non-EOHS patients on demographics, comorbidities, and hospital outcomes. Propensity score matching was used to evaluate the impact of EOHS on in-hospital mortality, length of stay (LOS), discharge disposition, and hospital charges. Multivariable logistic regression identified predictors of mortality among EOHS patients. Additional analyses assessed outcomes by procedure type, procedure�complication combinations, risk stratification, and temporal trends.
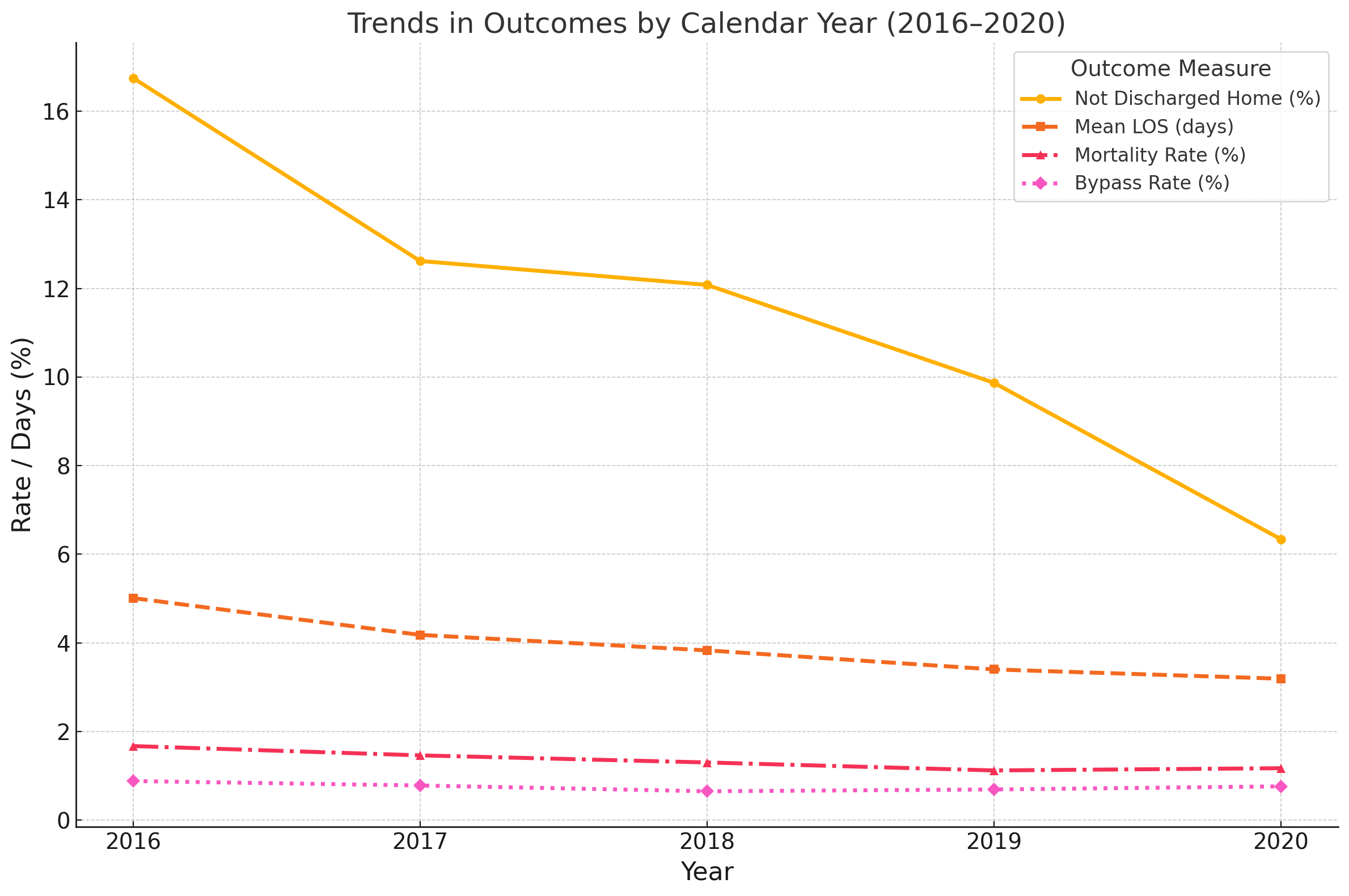
Results: Among 54,557 TAVR patients, 403 (0.74%) underwent EOHS. From 2016 to 2020, overall TAVR mortality declined (1.67% to 1.17%, p=0.0005), while EOHS incidence remained unchanged (~0.8%, p=0.471). EOHS patients were more often female (52.9% vs 44.4%, p=0.001) and younger (19.6% under age 70 vs 13.5%, p<0.001). In matched analysis, EOHS was associated with significantly higher mortality (31.1% vs 2.7%), longer LOS (16.3 vs 8.3 days), lower home discharge (63.5% vs 75.3%, p=0.001), and greater charges ($638K vs $292K; all p<0.001). Strongest predictors of EOHS mortality included intra-procedural cardiac arrest (OR 9.95), severe sepsis (OR 5.53), respiratory failure (OR 4.11), and acute kidney injury (OR 4.17). Valve repair (60%), pericardial procedures (54.5%), and valve replacement (37.8%) were the most lethal operations. Combinations such as valve replacement with subsequent development of respiratory failure (64.3%) and CABG with development of severe sepsis (100%) were particularly fatal. Risk stratification of the full TAVR cohort showed a stepwise mortality gradient: 0.42% in low-risk, 0.51% in medium-risk, and 2.94% in high-risk patients (p<0.001). EOHS mortality varied by hospital type: urban teaching hospitals had the highest rate (27.9%), followed by rural (20.0%) and urban non-teaching centers (15.6%). Bed size did not significantly affect mortality. Regional variation was also observed, with the South Atlantic having the highest EOHS rate.
Conclusion: EOHS during TAVR is rare but is associated with high mortality and healthcare burden. Institutional readiness, surgical backup capability, and proactive multidisciplinary planning may influence survival. Further investigation into device type, complication subtype, and institutional factors is warranted to guide preventive strategies and improve rescue success.
Table 1: Primary Open-Heart Procedures
| Procedure | Incidence | Mortality Rate (%) |
| Surgical Valve and Coronary Artery Dilation Procedures | 1 | 100 |
| Valve Repair | 10 | 60 |
| Cardiac Chamber and Pulmonary Vein Repair/Restriction | 11 | 54.5 |
| Surgical Cardiac Device Implantation | 9 | 44.4 |
| Anatomic Destruction and Valve Release Procedures | 5 | 40 |
| Valve Replacement | 37 | 37.8 |
| Supplementary Procedure | 22 | 31.8 |
| Excision of Intracardiac Material | 10 | 30 |
| CABG | 21 | 28.6 |
| Cardiac Device and Structure Extraction Procedures | 21 | 28.6 |
| Other Cardiac | 7 | 28.6 |
| Septal Defect | 27 | 25.9 |
| Pericardial Drainage Procedures | 46 | 15.2 |
| Atrial Appendage or Chamber Occlusion Procedures | 2 | 0 |