Back to 2025 Abstracts
Reasons for Delayed Hospital Discharge in Medically Ready Patients Following Elective Colorectal Surgery
Veer S. Sawhney
*, Sara Myers, Bachar Halimeh, Sing Chau Ng, Samantha J. Rivard, Jennifer Davids, Olga Beresneva
Surgery, Boston Medical Center, Boston, MA
BackgroundExtended postoperative LOS following elective colorectal surgery increases risk of hospital-acquired infections and deconditioning. Prolonged LOS may result in substantially higher costs for both patients and hospitals, as well as further contributing to inpatient bed shortages. While current literature suggests more comorbid individuals have longer LOS, reasons for delays in hospital discharge for patients who are medically ready are not well established.
MethodsWe conducted a single institution prospective study at an academic, urban, safety-net hospital. All patients from 3/2024-6/2024 and 12/2024-2/2025 admitted for an elective colorectal surgery with a planned inpatient stay of at least 1 day were included. Demographic information, patient comorbidities and diagnostic information were collected. Operative notes provided details on approach, anesthesia type, length of surgery, estimated blood loss, and complications. The dates patients were medically cleared for discharge and when they were actually discharged were noted. Patients discharged later than when they were medically cleared were considered a late discharge. Clinical team was interviewed to detail reasons for late discharge.
Results35 patients were included, of which half were male (51.4%). The median age was 57 (�IQR 47-68). 40% were black and 31.4% white, and 74.3% were non-Hispanic. Common comorbidities included hypertension (48.4%), Dyslipidemia (35.5%), Diabetes Mellitus Type II (19.4%), and History of Other Cancers (19.4%). Cancer (43%), Diverticulitis (20%), and Rectal Prolapse (11%) were the most frequent diagnoses. Surgical approach was evenly distributed between robotic (34%), laparoscopic (31%), and open (34%). The most common surgeries were colectomy (51%), ostomy reversal (17.1%) and rectopexy (11%).
29% of patients (n=10) were discharged later than when they were medically cleared. The most common reason for late discharge was patient preference to stay longer (60%). Other reasons included inadequate pain control, transportation issues, absence of an ostomy nurse for education over the weekend, and case management challenges with long-term care placement. Late discharge was not associated with age, sex, race, or operative approach in a fisher analysis (p>0.05).
ConclusionsThis study of patients with extended LOS following elective colorectal surgery identified nuanced social and logistical causes that are not typically documented in the electronic medical record. These results highlight a need to set expectations preoperatively with patients surrounding their expected LOS, as well as educating providers on the potential harms of extended LOS. Discharge planning and education in the preoperative period for both patients and providers, as well as identifying specific areas where additional resources will improve LOS measurably may help reduce non-medical extended LOS following colorectal surgery.
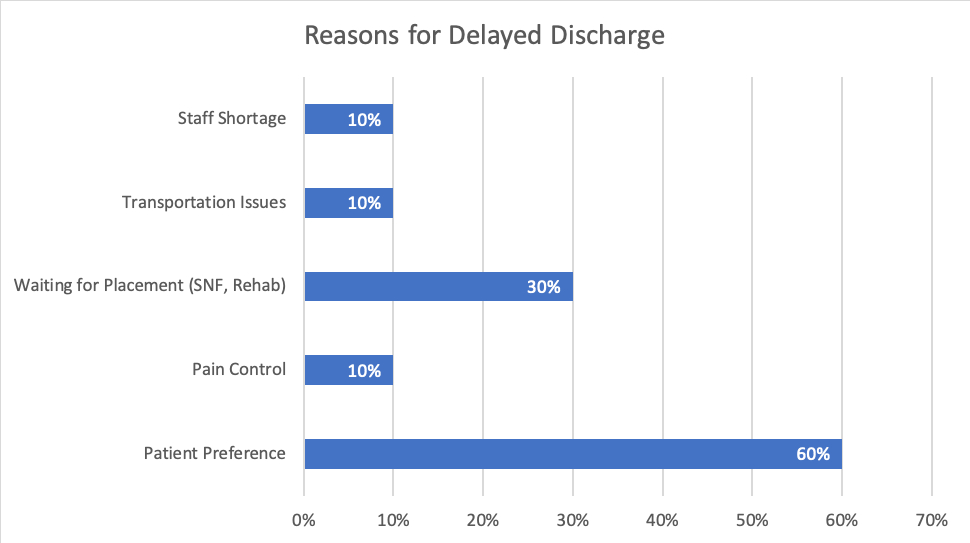
Figure 1. Frequency of Reasons Cited for Discharge Later Than Medical Clearance Date


