Back to 2025 Abstracts
A Systematic Review and Meta-Analysis of Perioperative Care Pathways in New Ileostomates: Can We Prevent Hospital Readmission?
Alice Jo
*, Sara W. Mayo
General Surgery, Dartmouth-Hitchcock Medical Center, Lebanon, NH
Background: Ileostomies, commonly performed for fecal diversion, are associated with high complication and readmission rates. Enhanced Recovery After Surgery (ERAS) protocols have successfully decreased overall morbidity and length of stay in elective colorectal surgical patients. ERAS protocols have not significantly impacted readmission rates related to ileostomy complications, highlighting the need for ileostomy-specific care pathways. This meta-analysis evaluates the effectiveness of perioperative ileostomy care pathways compared to standard care in reducing 30-day readmission rates.
Study Design: A systematic search of PubMed, Cochrane Library, and CINAHL was conducted for studies published from January 1, 2010, to January 1, 2024. Included studies met the following criteria: (1) randomized controlled trials (RCTs), quasi-experimental studies (including quality improvement projects and before-and-after studies), or prospective/retrospective cohort studies; (2) patients aged ?18 years undergoing new ileostomy creation; (3) interventions specifying perioperative ileostomy pathways alongside usual ERAS-based care; (4) studies reporting 30-day readmission rates as primary or secondary outcomes; and (5) publications in English. Risk of bias was assessed using the Cochrane Risk of Bias Tool 2.0 for RCTs and the ROBINS-I tool for non-RCT studies (PROSPERO ID: CRD42024567847)
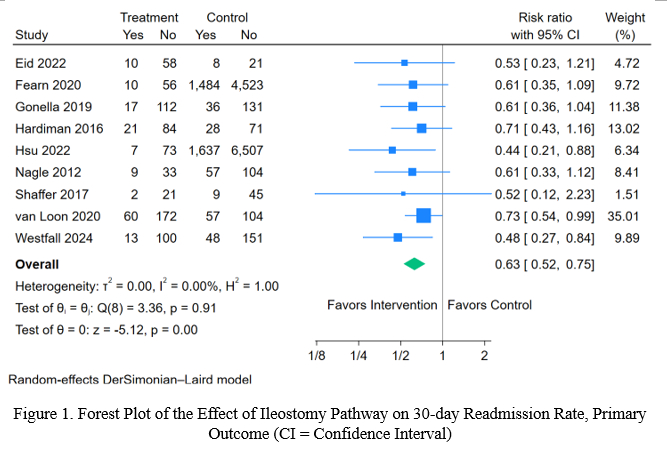
Results: Of 1,565 studies initially identified, title and abstract screening narrowed the selection to 35 studies for full-text review, with 9 studies meeting inclusion criteria for quantitative analysis. The 9 studies analyzed employed non-randomized designs and included three key components in their ileostomy pathways: (1) patient empowerment, (2) intake and output monitoring, and (3) increased postoperative surveillance. Meta-analysis of the primary outcome demonstrated significantly reduced 30-day readmission rates (RR 0.63, 95% CI 0.52–0.75) (
Figure 1). The secondary outcome, 30-day readmission rates specifically due to dehydration, showed a significant decrease (RR 0.37, 95% CI 0.24–0.55). Analysis demonstrated no difference in length of stay (mean difference ?0.06 days, 95% CI ?0.21 to 0.10).
Conclusions: Perioperative ileostomy pathways that incorporate (1) patient empowerment, (2) intake and output monitoring, and (3) increased postoperative surveillance are associated with significantly reduced 30-day readmission rates overall and specifically due to dehydration, without prolonging hospital stays. These findings emphasize the benefits of utilizing ileostomy-specific care pathways to improve patient care.