Back to 2025 Abstracts
Reliability of White Light Scan Technology for Evaluation of Vacuum Bell Therapy in Pectus Excavatum
Sara Lee
*, P. Nina Scalise, Megan Z. Chiu, Donna C. Koo, Kelly Bartkus, Farokh Demehri
Department of General Surgery, Boston Children's Hospital, Boston, MA
BackgroundThe Haller Index (HI) derived from chest radiography (CXR) or computed tomography (CT) is the standard for measuring severity of pectus excavatum (PE). Non-surgical correction of PE for appropriate candidates is done with vacuum bell (VB) therapy. VB can require prolonged treatment with gradual change in chest wall geometry. The improvement is measured by the depth of the sternal depression from the anterior chest wall, or funnel depth (FD). To better mirror radiography without repeated exposure to radiation, we sought to assess the reliability of a handheld 3D White Light Scanner (WLS) to evaluate response to vacuum bell treatment and compare WLS-derived indices to the conventional radiographic HI and FD.
Study DesignA retrospective review from April 2022 to December 2024 was performed of pectus excavatum patients who started VB therapy at a single institution. White light scans were performed before initiating therapy and at every subsequent clinic visit after starting VB therapy. Two measurements were derived from the scan: 1) a WLS-derived “external” Haller index (WLS_EHI) was calculated by dividing the mediolateral diameter by the anteroposterior diameter of an axial cross-section through the chest at the deepest point of PE depression (ML/AP in Figure 1) and 2) a novel WLS-derived maximal funnel depth (WLS_FD) was calculated as the distance between the deepest point of the depression and a coronal plane across the anterior portion of the chest (FD in Figure 1). Paired t-tests were used to evaluate the response of funnel depth to VB therapy. Pearson regression analysis assessed correlation between CXR-derived HI, provider-measured Pectus Excavatum Depth (PED), WLS_EHI, and WLS_FD.
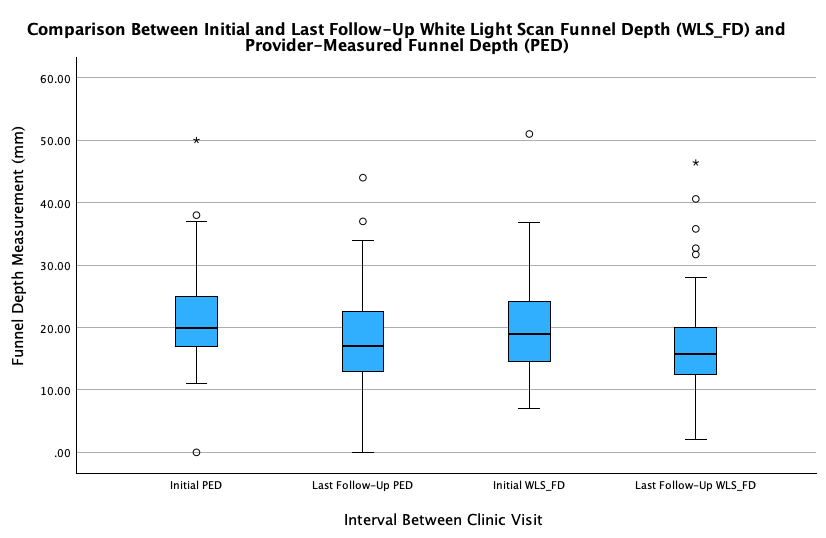
ResultsFifty patients who had both initial and follow-up WLS were included. They had an average time to last follow-up of 9.8 months. The cohort consisted of 43 (86%) males, median age of 14 years (IQR 12-15), median BMI of 18.2 (IQR 16.9-19.9) and median initial HI of 3.5 (IQR 3-4.1). Eight patients had increased PE defect of 13.5% on WLS_FD. There was a significant mean decrease of 3.5 ± 4.5mm (N=35; p<0.05), or an average of 20.5% in PED. This corresponded to a significant mean decrease of 3.2 ± 4.5mm (N=50; p<0.05) or an average of 21.3% in WLS_FD (Figure 2). WLS_PD is strongly correlated to PED (r = 0.86, p<0.05) and weakly with HI (r=0.36, p <0.05). WLS_EHI had the strongest correlation to HI (r=0.52, p <0.05) and there was a significant decrease in mean WLS_EHI of 0.44 ± 1.1mm (N=43; p<0.05).
ConclusionWLS measurements reliably showed an improvement in funnel depth during the use of VB therapy. The strongest correlation to the traditional HI was WLS-derived external HI and the overall strongest correlation was between WLS-derived funnel depth and physician-measured PED. Our cohort suggests WLS is a feasible way of objectively quantifying the severity of PE deformities and reliably monitoring defect progression in response to vacuum bell therapy.
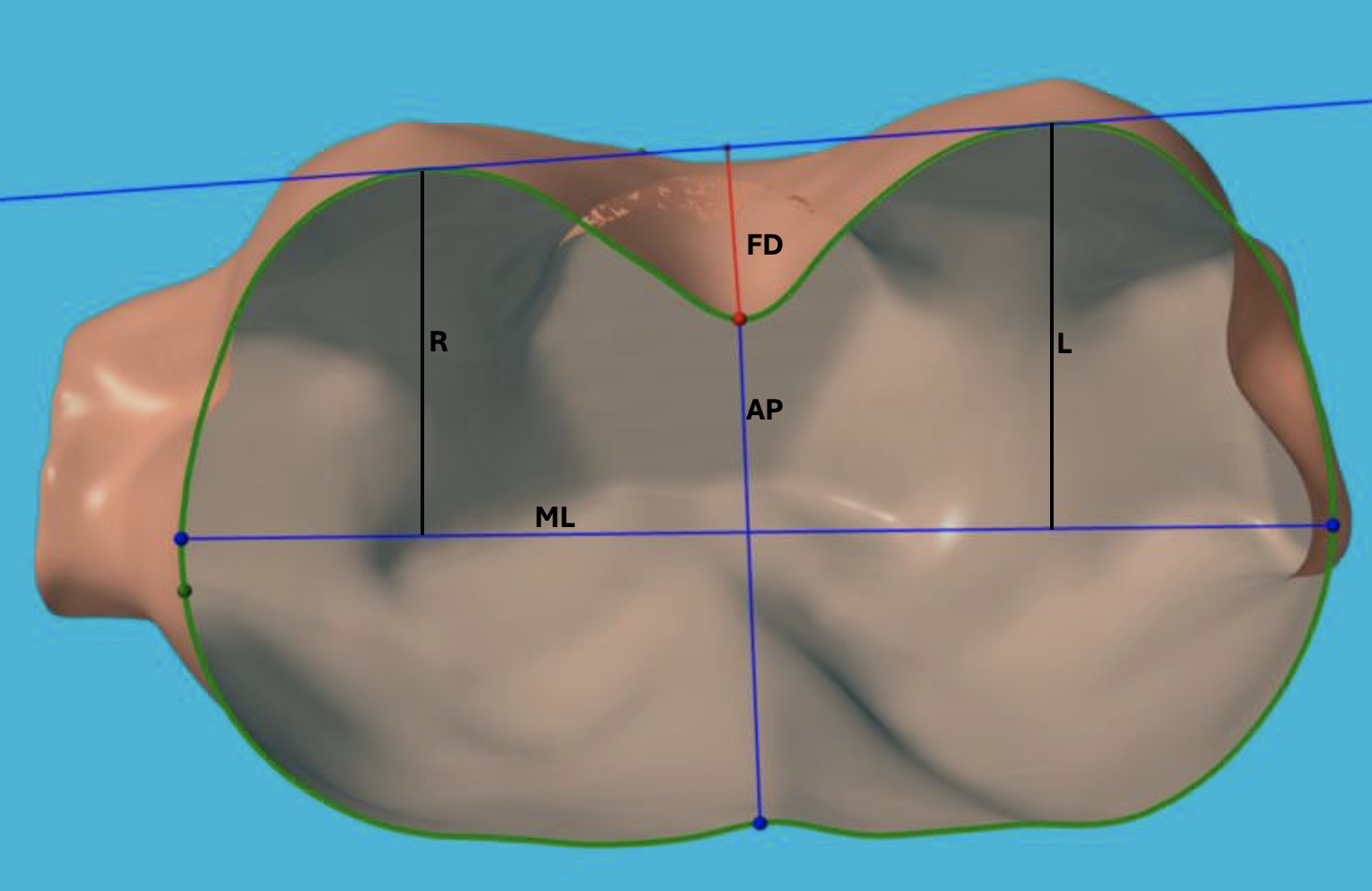
Figure 1. White Light Scan Reconstruction with Labels on Derived Measurements. EHI = ML/AP and WLS_FD = FD.