Back to 2025 Abstracts
Incidence of the Development of Rectal Prolapse after Surgical Repair of Pelvic Organ Prolapse
Laura Palmere
*1, Kris Strohbehn
1, Sara W. Mayo
21Urogynecology and Reconstructive Pelvic Surgery, Dartmouth Hitchcock, Lebanon, NH; 2Colorectal Surgery, Dartmouth Hitchcock, Lebanon, NH
Background: Pelvic organ prolapse (POP) is a common condition among aging women, while rectal prolapse (RP) is not Both conditions have similar risk factors, but there has been little research suggesting that surgical repair of POP may be a risk factor in the development of de novo RP. The anatomy of the pelvic floor is shifted in women who undergo surgical management of POP, and this change of the vector of downward force may contribute to the development of RP. Our objective is to determine the incidence of RP noted after surgical repair of POP at a single institution.
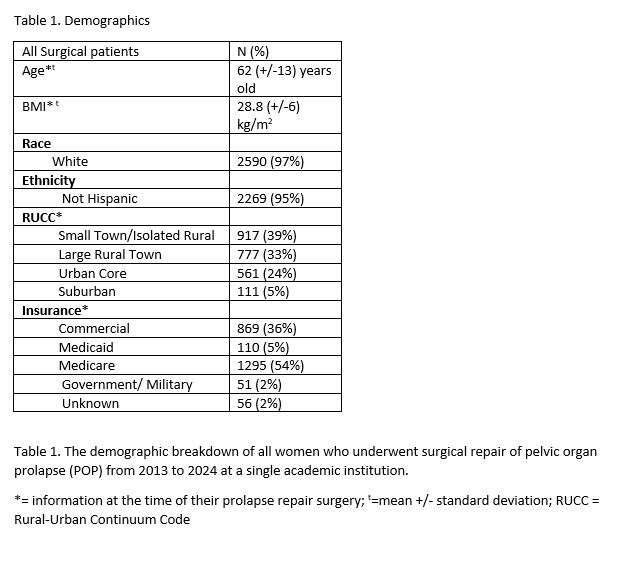
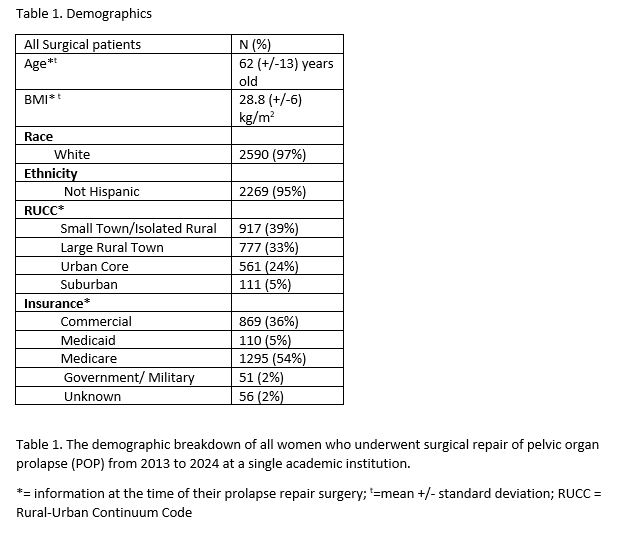
Study Design: Retrospective chart review from 2013 to 2024 of women who underwent surgical management for POP at a single institution. Demographic variables were analyzed (table 1). Charts of patients who were diagnosed with RP were reviewed to validate the correct diagnosis and time interval to the diagnosis of RP from their index POP repair surgery. Statistical analysis with chi-squared testing with a significance set at a probability value of <=0.05. Logistic regression was used to assess the impact the surgical type on the development of RP, controlling for age and BMI. Institutional Review Board approval was obtained prior to the start of the study.
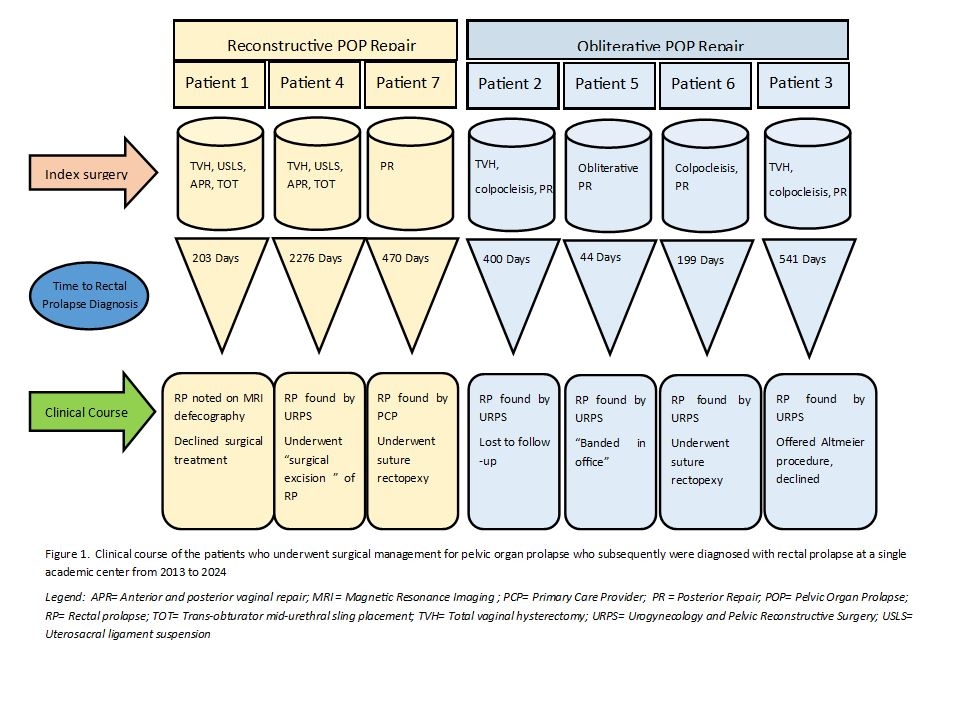
Results: 2,381 surgeries as management for POP were performed (2,150 reconstructive and 231 obliterative) (Table 2). Seven patients developed RP after their index surgery, and four of these patients chose to undergo subsequent surgery to correct RP. Three of these patients had a reconstructive surgical approach, while four had an obliterative vaginal surgery (0.14% reconstructive vs. 1.7% obliterative, p<0.05, table 2, figure 1). Although age alone was not a predictive factor in the development of RP in this patient cohort, women who chose obliterative repairs tended to be older than those who chose reconstructive repairs (mean 75 vs. 61 years old respectively, p<0.05. Table 1). Using a logistic regression model to control for age and BMI, patients who underwent obliterative surgical repair had a higher odd of developing RP than those who underwent reconstructive repair (OR 13.1, 95% CI 2.4-70.7, p<0.05). There was no statistical difference in the incidence of developing RP after POP surgery based on race, ethnicity, insurance type, or Rural-Urban Continuum Codes (RUCC). The time from surgery to the diagnosis of RP did not follow a trend based on the index surgery type. (Figure 1)
Conclusions: While rare, obliterative surgical management for POP may increase the likelihood that a patient develops RP, compared to reconstructive surgical management. Patients who choose obliterative repair tend to be older than their counterparts who choose reconstructive repair, however age was not found to be a contributing factor to the development of RP in this cohort. Further research is needed to understand the relationship between the development of RP after POP repair surgery.