Back to 2025 Abstracts
Patterns of Firearm Injury Across a Rural State: A 10-Year Single Center Experience
Lucero G. Paredes
*, Carolyne Falank, Bryan C. Morse, Christopher G. Turner
Surgery, Maine Medical Center, Portland, ME
Background: Firearm injuries remain a significant cause of morbidity and mortality, particularly among rural communities. Though Maine has a higher-than-average firearm suicide rate, little is known about the extent of firearm injury across the state. As the only Level 1 Trauma Center in Maine, we sought to describe patterns of firearm injury presenting to our institution and compare differences in outcomes across three common intentions: self-harm, assault, and accidental.
Methods: We queried our institution’s trauma registry for all individuals who presented with a firearm injury from 2015-2024. Individual variables assessed include demographic characteristics (age group [< 18, 18-39, 40-64, and ? 65 years], race/ethnicity, sex, rurality), insurance status, New Injury Severity Score (NISS), Emergency Department (ED) disposition, and in-hospital mortality. Rurality was determined using federal Rural-Urban Commuting Area codes, a classification system based on zip code. Patients were stratified by intention and compared using Kruskal Wallis test for continuous variables and Pearson ?2 test for categorical variables.
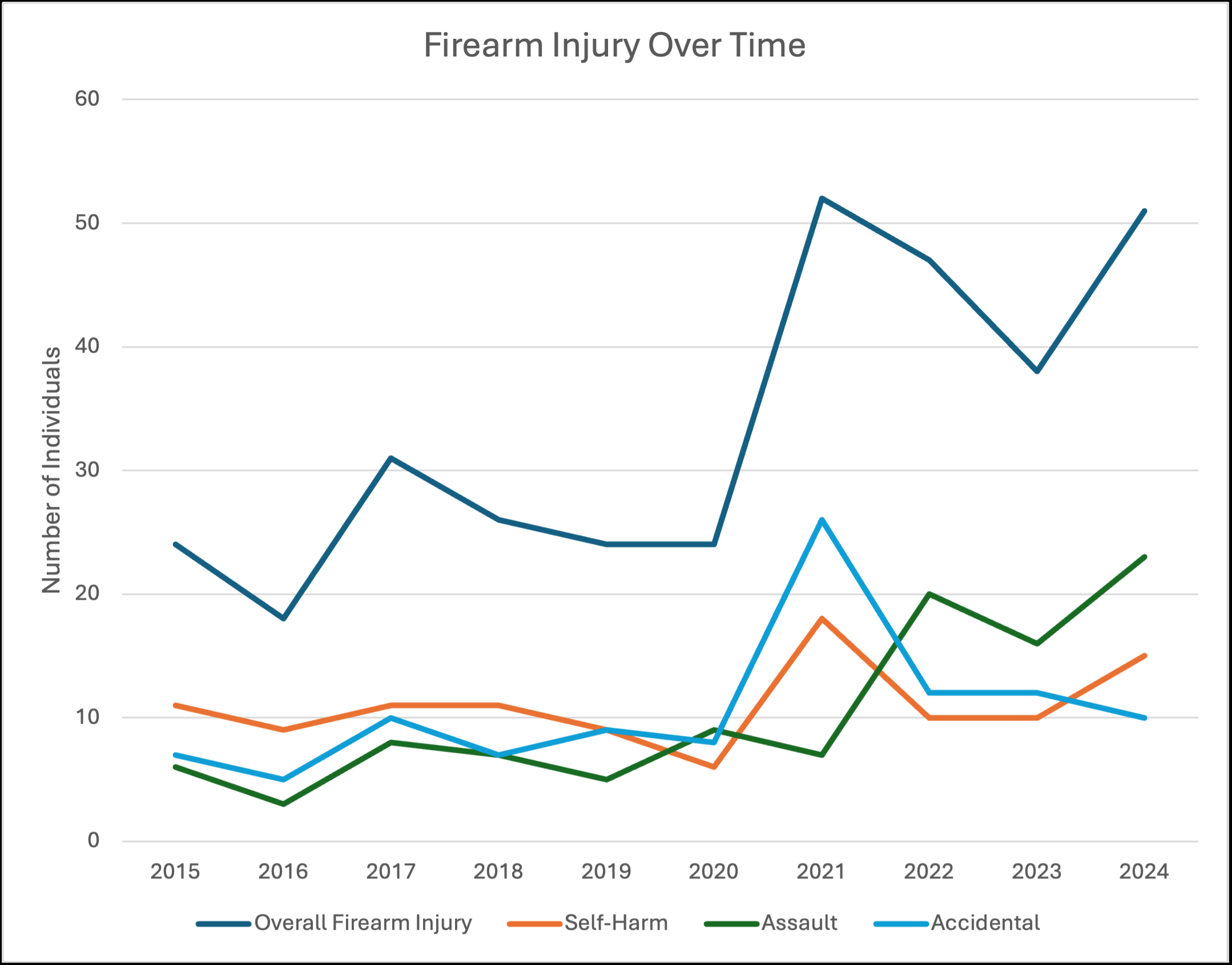
Results: A total of 335 patients presented to our trauma center with a firearm injury from 2015-2024. 280 were male [83.6%], 283 white [84.5%], with median [IQR] age, 34 [23-53] years; half (58.6%) were from a rural zip code. Overall, in-hospital mortality rate was 21.8%. Intentions included self-harm (110, 32.8%), accidental (106, 31.6%), assault (104, 31.0%), legal intervention (10, 3%), and undetermined (5, 1.5%). Across the three leading intentions (n=320), patients with self-harm injuries were more likely to be in the two oldest age groups (?40 years), from a rural zip code, injured in the head or neck, and require the intensive care unit (p<.001 for all). Patients with assault injuries were more likely to be in the 18–39-year age group, non-White, from an urban zip code, and injured in the chest and abdomen (p<.001 for all). Patients with accidental injuries were more likely to be in the youngest age group (<18 years), injured in an extremity, and discharged from the ED (p<.001). Average in-hospital mortality rates, excluding those who died in the ED, differed across intention (p<.001), 42.6% for self-harm, 5.1% for assault, and 1% for accidental. The number of patients presenting following firearm injury increased over the study period, with the largest increase in assault (Figure 1).
Conclusion: In this single center study, distinct demographic and outcome patterns were identified across the intentions of self-harm, assault and accidental injury. Further studies are needed to define risk factors and establish potential interventions for reducing firearm injury across this rural state.