Back to 2025 Abstracts
Reflections and Lessons Learned from a Mass Shooting in Lewiston, Maine
Christoph A. Niederhauser
*1, Tammy Lachance
2, Timothy C. Counihan
21University of New England College of Osteopathic Medicine, Biddeford, ME; 2Central Maine Medical Center, Lewiston, ME
BackgroundOn October 25, 2023, a mass shooting at two locations in Lewiston, Maine claimed 18 lives, making it the deadliest mass shooting in Maine and the 10th worst in U.S. history. This mass casualty incident (MCI) is analyzed from the perspective of Central Maine Medical Center (CMMC), an ACS Level 3 Trauma Center, to help other hospitals better prepare for future MCIs.
Study DesignHospital operational and clinical records, policies, MCI debriefing meetings, and the official investigative report were retrospectively reviewed.
ResultsThis MCI produced 31 trauma victims at two locations within 15 minutes. Fifteen victims died at the scene, 15 were transported to hospitals, and one was treated on-site. Within 20 minutes, 14 critically injured patients arrived at CMMC, overwhelming available resources. The hospital disaster plan was enacted. All available hospital staff were contacted (surgeons, nurses, OR technologists, anesthesia providers, etc.) and many team members reported to care for the victims. One patient was taken to a nearby hospital. The victims aged 16 to 76, with 11 males and three females.
Initial triage was ineffective, resulting in numerous patients being misregistered, missing initial trauma bloodwork, and being assigned to the wrong hospital floor. Emergency Department resuscitation included Mass Transfusion Protocol (MTP) for three patients and standard blood transfusions for two, with a total of 63 blood product units administered. Resuscitation was complicated by a critical shortage of blood products at CMMC, necessitating emergency blood transfers from other hospitals via helicopter due to a citywide lockdown. An influx of victim family members overwhelmed case management and required an ad hoc system to be devised.
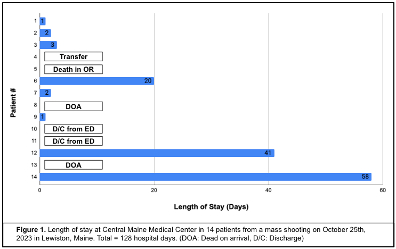
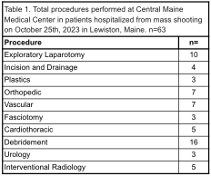
Two patients were pronounced dead on arrival. Eight patients underwent emergency surgery, one of whom died in the operating room from a vena cava injury. Three required ICU care, one was transferred to another hospital, and three were discharged after short stays (Figure 1). Patients spent 128 total hospital days of which 103 were ICU days. Sixty-three invasive procedures were performed (Table 1). All victims were offered virtual mental health care once stable.
ConclusionsLessons learned included: Utilizing established triage protocols can prevent bottlenecks and patient identification and placement errors. Regular updates to policies, staff training, and family involvement protocols will help maintain readiness. A robust plan should address not only the event but the subsequent impact on the system for days and weeks after. System-wide blood bank plans worked to keep a steady blood supply to the facility. Mental health resources need to be available for victims and team members soon after an event. Ultimately, a well-staffed and equipped Level 3 Trauma Center can care effectively for a large MCI.