Back to 2025 Abstracts
Validation of prognostic impact of extramural vascular invasion in colorectal cancer across multiple racially distinct international cohorts
Swati Sonal
*3, Susan McKendry
4, Akiyoshi Ikebata
2, Kohei Shigeta
2, Koji Okabayashi
2, Miho Kawaida
6, Hajime Okita
6, Rama Al Masri
5, Mahmoud Al Masri
5, Paul Richardson
1, Robert Goldstone
1, Hiroko Kunitake
1, David L. Berger
11General and GI Surgery, Massachusetts General Hospital, Boston, MA; 2Surgery, Keio University School of Medicine, Tokyo, Japan; 3Surgery, University of Minnesota Medical School, Minneapolis, MN; 4Surgery, Queen's university Belfast, Belfast, Northern Ireland, United Kingdom; 5Surgery, King Hussein Cancer Center, Amman, Jordan; 6Diagnostic Pathology, Keio University School of Medicine, Tokyo, Japan
Introduction:
Extramural vascular invasion (EMVI) is a known poor prognostic factor in colorectal cancer (CRC) in the United States (US). Our primary objective was to validate the prognostic impact of EMVI in stage II and III colon cancer and assess the effect of adjuvant therapy in EMVI-positive tumors in US and Japan cohorts. The secondary objective was to assess the prognostic impact of EMVI in colon and rectal cancer in Jordan.
Methods:
Patient records were acquired retrospectively from IRB-approved databases at three tertiary care institutions across the US, Japan, and Jordan. Patients who underwent curative resection for Stage II & III colon adenocarcinoma in the US (N=770, 2004-2018) and Japan (N=426, 2012-2019) were included as were patients undergoing resection for Stage I-IV colorectal cancer in Jordan (N=868, 2015-2022). Overall survival (OS), disease-free survival (DFS), and time to recurrence (TTR) were assessed using the Kaplan-Meier method. Multivariable analysis was performed using the Cox regression model to assess the effect of EMVI on recurrence and survival, while adjusting for age, race, BMI, ASA score, surgical admission type, bowel obstruction, tumor location, grade, extent of invasion, lymph node metastasis, perineural invasion, and adjuvant chemotherapy. Proportional hazard assumption was examined using Schoenfield residuals and time-dependent covariate analysis was done as appropriate if Cox model violated the assumption.
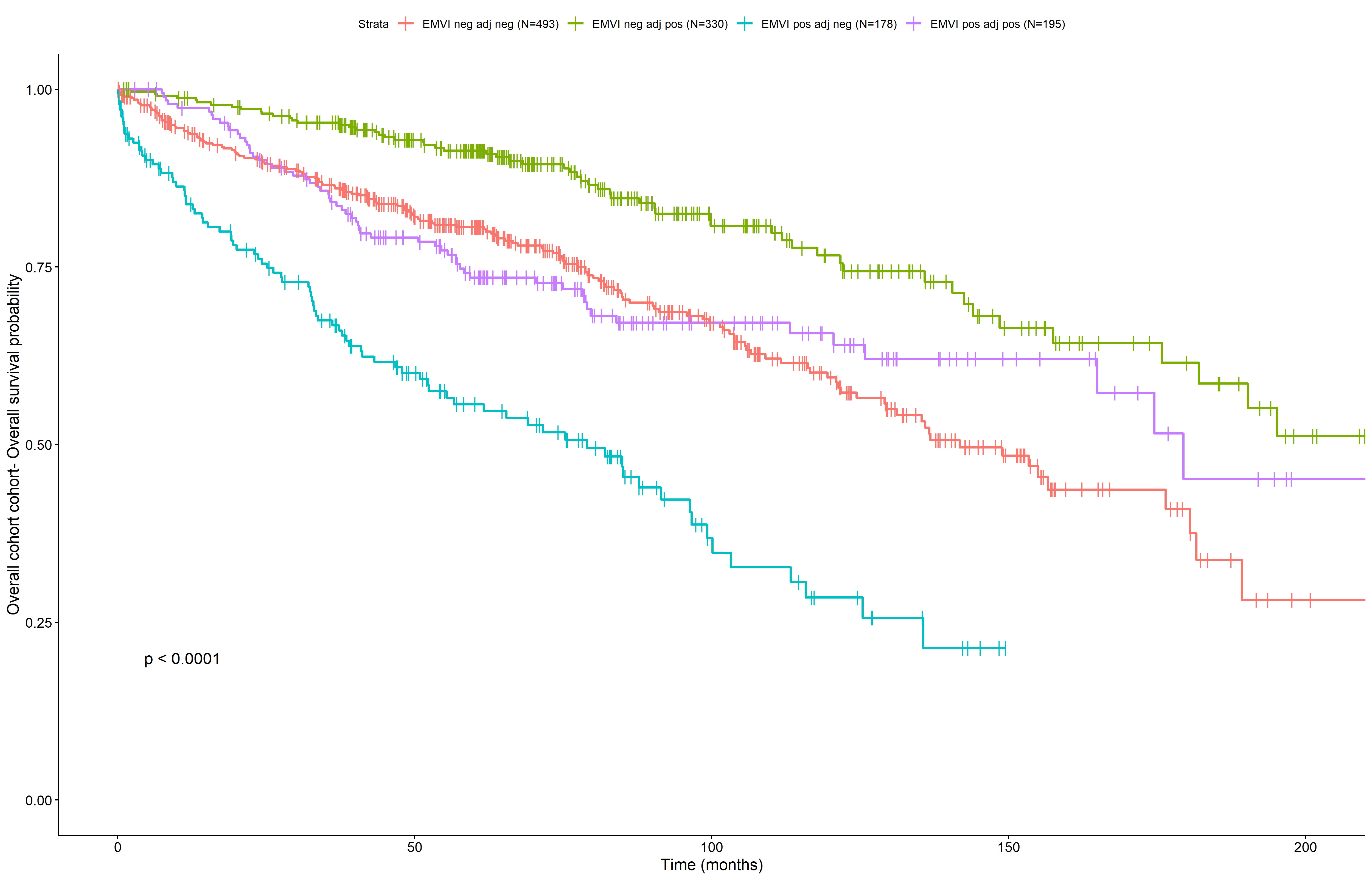
Results:There were 251/770 (32.6%), 122/426 (28.6%), and 89/868 (10.3%) EMVI positive tumors in the US, Japan, and Jordan cohorts respectively. EMVI positivity was associated with a higher grade, extent of invasion, higher rates of perineural invasion, lymph node metastasis, adjuvant therapy, and worse OS, DFS, and TTR on univariable analysis (p<0.05) across all three cohorts. Combined multivariable analysis performed for US/Japan demonstrated that EMVI was an independent poor prognostic factor for OS (Hazard ratio, HR 1.68, 95% CI 1.32-2.15), DFS (HR 1.96, 1.42-2.69 for <14 months; HR 2.27, 1.55-3.31 for 14-41 months) and TTR (HR 1.94, HR 1.44-2.62) while adjusting for covariates. Patients with EMVI-positive tumors who did not receive adjuvant chemotherapy had worse OS (HR: 1.87, 1.12-3.09) and DFS (HR: 1.45, CI: 0.93– 2.27), but similar TTR compared to those who received adjuvant chemotherapy, while adjusted for covariates. Multivariable analysis performed for Jordan cohort failed to demonstrate any significant prognostic impact of EMVI on OS, DFS, and TTR, likely due to small sample size.
Conclusion:
EMVI is an independent prognostic indicator for colorectal cancer, especially non-metastatic colon adenocarcinoma across geographically and racially distinct cohorts. Adjuvant chemotherapy improves survival in EMVI-positive tumors and should be considered for these tumors independent of tumor stage.