Back to 2025 Abstracts
Examining Maternal Health and Socioeconomic Drivers Associated with Necrotizing Enterocolitis in a Safety Net Hospital
Abdimajid Mohamed
*1, Bharath Miriyam
2, Rachel Allen
3, Christopher Muratore
11Pediatric Surgery, Boston Medical Center, Boston, MA; 2Boston University, Boston, MA; 3Boston University School of Medicine, Boston, MA
Introduction:Necrotizing enterocolitis (NEC) is a severe gastrointestinal disease predominantly affecting preterm infants, with significant morbidity and mortality. While prematurity is a well-established risk factor, the impact of maternal health disparities and social determinants of health (SDOH) on NEC severity remains poorly characterized. This study examines associations between maternal comorbidities, socioeconomic factors, and NEC outcomes in a high-risk population at a safety-net hospital.
Methods:This retrospective cohort study included 59 infants born between 2015 and 2022, diagnosed with NEC and classified by Modified Bell staging: 1A/1B, 2A/2B, and 3A/3B. Maternal comorbidities, delivery characteristics, and SDOH variables were extracted from electronic medical records and supplemented with American Community Survey (ACS) data. Statistical analyses, including chi-square and Fisher�s exact tests, assessed associations between NEC severity and maternal/infant characteristics. Socioeconomic indicators were evaluated using the Childhood Opportunity Index (COI). This study received institutional review board approval.
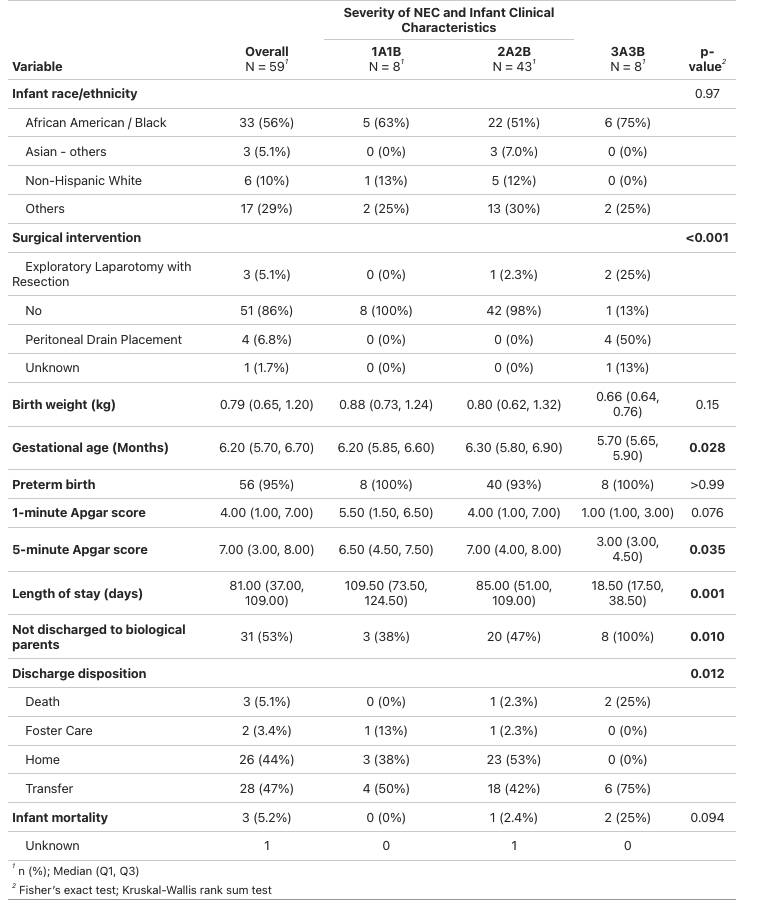
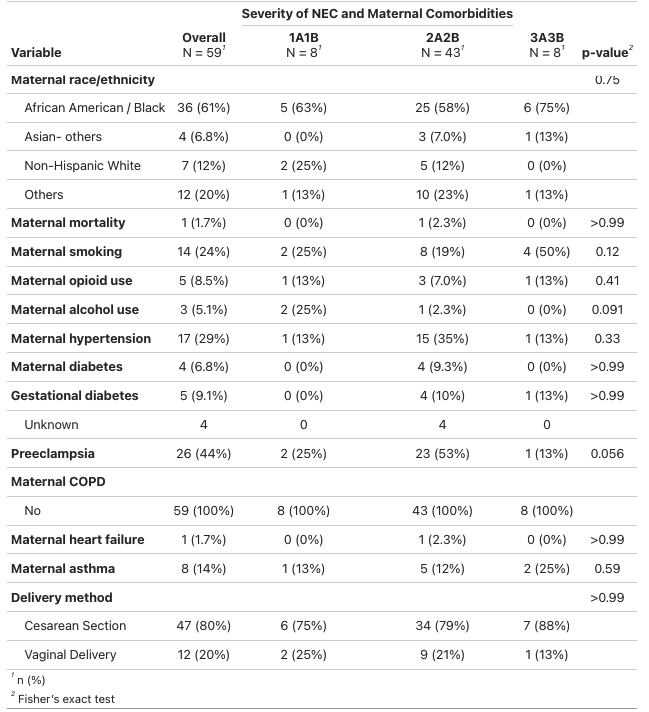
Results:Among 59 NEC-affected infants, 8 (13.5%) were 1A/1B, 43 (73%) were 2A/2B, and 8 (13.5%) were 3A/3B. There were 3 (5.1%) neonatal deaths and 1 (1.7%) maternal death. The majority (56%) were Black. Maternal hypertension (29%) and preeclampsia (44%) were common. Maternal smoking was more prevalent in severe NEC (50% in 3A/3B vs. 24% overall, p=0.12). Maternal opioid use (8.5%), alcohol use (5.1%), and diabetes (6.8%) were observed but did not significantly differ by NEC severity.
Surgical intervention was required in 7 infants: 3 (5.1%) underwent laparotomy with bowel resection, and 4 (6.8%) had peritoneal drainage. Discharge outcomes showed 53% of NEC-affected infants were discharged without their biological parents.
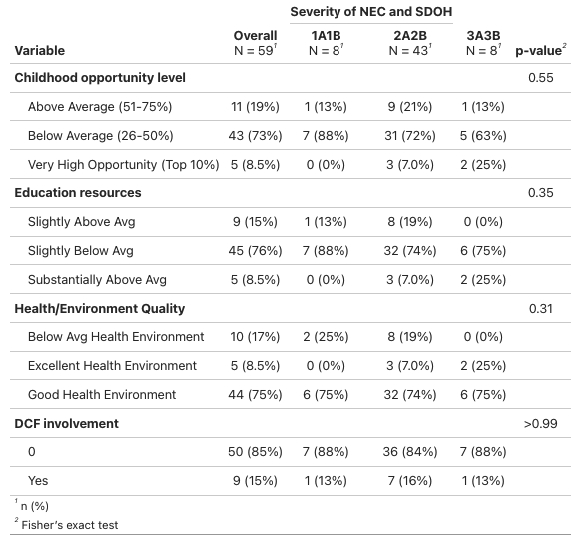
SDOH analysis revealed 73% of affected infants were born in neighborhoods with below-average childhood opportunity levels. Additionally, 76% of mothers lived in areas with slightly below-average educational resources, and 17% in areas with below-average health/environmental quality.
Conclusion:Significant maternal and socioeconomic disparities exist among NEC-affected infants. Maternal hypertension, smoking, and preeclampsia were prevalent, particularly in severe cases. Adverse socioeconomic factors, including low childhood opportunity levels and reduced educational resources, were common. These findings highlight the critical role of maternal health and socioeconomic conditions in NEC severity, underscoring the need for targeted public health interventions to mitigate maternal risk factors and improve neonatal outcomes.