Back to 2025 Abstracts
Surgical Antibiotic Prophylaxis for Elective Pancreatoduodenectomy: A Propensity Score–Weighted Comparative Analysis
Kaique Filardi
*, Oscar Serrano
Surgery, Hartford Hospital, Farmington, CT
Background. Pancreatoduodenectomy (PD) is a morbid procedure often associated with high rates of postoperative infectious complications, contributing to worse prognosis, increased length of stay (LOS), and mortality. The choice of surgical prophylaxis antibiotics is still debated. We sought to investigate the optimal antibiotic prophylaxis for PD patients.
Study design. The American College of Surgeons National Surgical Quality Improvement Project (ACS–NSQIP) pancreas-targeted database (2016–2023) was queried to identify patients who had an elective PD and the antibiotics prescribed prophylactically. Three cohorts were compared based on antibiotics used: first-generation cephalosporin (FC), second and third-generation cephalosporins (STC), and broad-spectrum (BS) antibiotics. Our primary outcome was surgical site infection (superficial, deep, and/or organ/space), nosocomial infections, and
Clostridium difficile colitis. As a secondary outcome, we evaluated the association between antibiotic choice and postoperative pancreatic fistula (POPF),30-day readmission,30-day reoperation,30-day mortality, and major complications. Patients who were preoperatively classified as ASA V or had an unknown antibiotic type were excluded. Inverse probability weighting using multinomial propensity scores was applied to balance antibiotic groups. We performed weighted logistic regression for each infection-related outcome. Adjusted predicted probabilities and pairwise risk differences were analyzed to compare groups while accounting for confounding.
Results. We identified 34,777 PD patients;31.4% received FC,27.3% STC,and 41.4% BS. The sample comprised 46% of females with an average age of 67 years. The adjusted probability of any Surgical Site Infection (SSI) was 25.3% (24.5%–26.1%), 23.5% (22.6%–24.5%), and 21.3% (20.6%–22.0%) for FC,STC, and BS, respectively. BS antibiotics consistently showed a statistically significant risk reduction difference in any SSI, postoperative sepsis, and pneumonia. Conversely, the adjusted probability analysis of secondary outcomes, including POPF (21.1%vs19.1%vs19.1%),30-day readmission (17.4%vs17.7%vs17.3%),30-day reoperation (5.2%vs5.1%vs5.1%), 30-day mortality (1.84%vs1.78%vs1.62%),and major complications (8.6%vs8.01%vs8.23%) remained similar across groups. Interestingly, infectious complications were most marked between the antibiotic groups when patients were stratified according to the preoperative biliary drainage method (no drain 23.3% vs drain 19.7%). Despite broader antimicrobial coverage, the incidence of
C difficile colitis remained very low and did not vary clinically among groups (1.21%vs1.89%vs1.63%).
Conclusion. Broader antibiotic prophylactic in elective PD patients yields improved patient outcomes, lowering rates of postoperative infections without increasing the clinical risk of
C difficile colitis. Furthermore, this advantage is most significant in patients whose biliary tree has been instrumented.
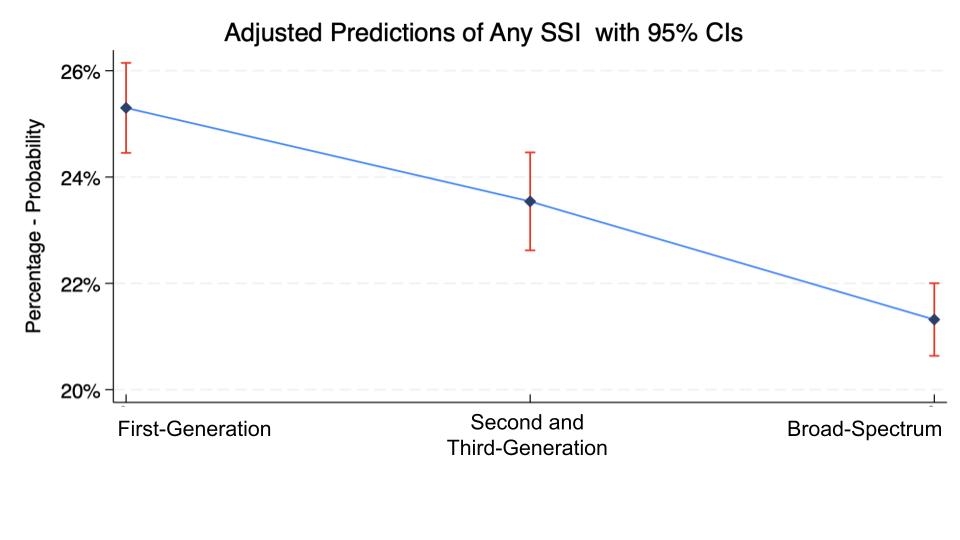 Adjusted Probability of Any SSI
Adjusted Probability of Any SSI 

