Back to 2025 Abstracts
Variations in Management of Blunt Splenic Injury by Hospital Training Status
Zane J. Hellmann
*, Carly Thaxton, Alexis Jones, Emily R. Christison-Lagay, Daniel G. Solomon
Surgery, Yale School of Medicine, New Haven, CT
Introduction:
Pediatric trauma surgeons have been the vanguard of non-operative management of hemodynamically stable or transfusion responsive patients with blunt splenic injury, establishing non-operative management as the contemporary standard of care. However, the threshold for identifying failure of non-operative management is not fully objective and can lead to variability in management strategies across institutions. We hypothesized that trauma centers with a pediatric surgical fellowships more rapidly adopt current consensus recommendations and be less likely to surgically intervene on blunt splenic injuries as compared to those institutions without pediatric surgery fellowships.
Methods:
The Pediatric Health Information System (PHIS) database is a repository for administrative data for 49 free-standing children�s hospitals. It was queried for all patients 18 years old or younger admitted with splenic injuries between 2016-2023 based on ICD-10 diagnostic codes. Patients were excluded from the study if a penetrating mechanism code was associated with the admission. ICD-10 diagnostic codes were used to calculate a surrogate of injury severity score (ISS). Splenic surgery or embolization was identified by ICD-10-PCS code during the index admission.
Results:
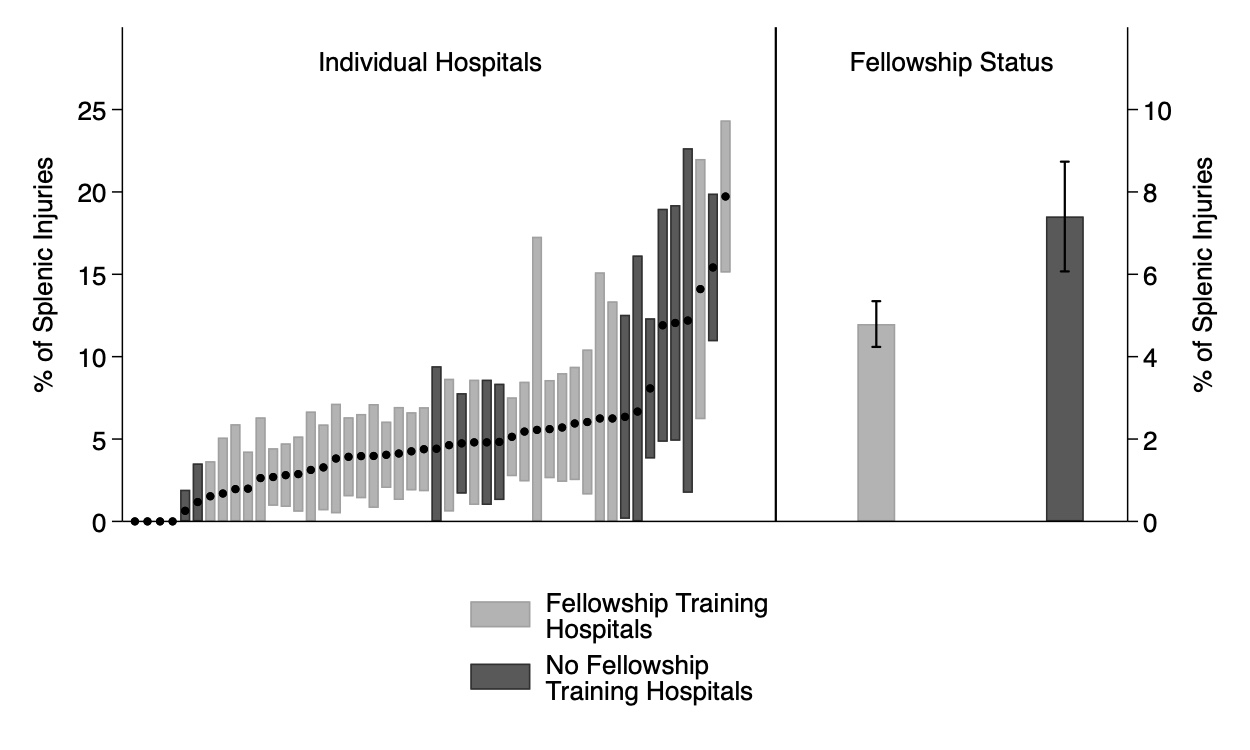
There were 7,183 patients identified with blunt splenic injury of whom 383 (5.3%) underwent surgical intervention or embolization. Patients treated at hospitals with or without a pediatric surgery fellowship were of similar ages, distribution of female, proportion white, and had similar calculated ISS. Patients treated at non-fellowship hospitals were more likely to have a major splenic laceration (30.1% vs 26.8
, p=0.01 and were more likely to die during their admission (3.7% vs 2.6%, p=0.02). Univariate analysis demonstrated that patients treated at hospitals with a pediatric surgery fellowship were less likely to undergo splenic intervention (OR 0.62, 95% CI 0.50-0.79, Figure 1). Multivariable logistic regression, controlling for calculated age, sex, race, payor status, calculated ISS, severity of splenic laceration, and total number of patients treated with splenic injuries at the hospital during the study period, demonstrated that patients treated at hospitals with a pediatric surgery fellowship were less likely to undergo a surgical procedure (OR 0.58, 95% CI 0.45-0.75).
Conclusion:
Despite national guidelines put forward by trauma and pediatric societies, there remains significant variation among hospitals regarding proportion of patients who undergo surgical procedures for treating splenic injury. This study suggests that institutions with pediatric surgery fellowships are less likely to perform splenectomy for splenic injury holding ISS, severity of splenic injury, and demographics constant.