
Should Lymph Node Harvest Impact the Decision to Administer Adjuvant Chemotherapy for High-Risk T3N0 Colon Cancer?
Vanessa M. Welten, Adam C. Fields, Annabelle Jones, Nelya Melnitchouk, James Yoo, Jennifer Irani, Ronald Bleday, Joel E. Goldberg
Brigham and Women's Hospital, Boston, Massachusetts, United States
Objective: The role of adjuvant chemotherapy in stage II colon cancer remains under investigation and in some cases remains controversial. Current guidelines recommend adjuvant chemotherapy for patients with stage II colon cancer with high-risk features, including, lymphovascular invasion (LVI) and poor differentiation. Although complete pathologic staging requires 12 lymph nodes for assessment, it is unknown whether an increased negative lymph node harvest portends improved survival in these high-risk patients possibly eliminating the need for adjuvant chemotherapy. This study aimed to determine the prognostic value of additional lymph node harvest for patients with T3N0 colon cancer with some high-risk features (poor differentiation and LVI).
Design: This is a retrospective study using the National Cancer Database (2004-2016).
Patients: Patients with stage II colon cancer (pT3N0) who had poor differentiation and LVI were identified.
Main Outcome Measures: The primary outcome was overall survival. Survival analyses were performed with log-rank tests and a cox-proportional hazards model was used to identify risk factors for survival.
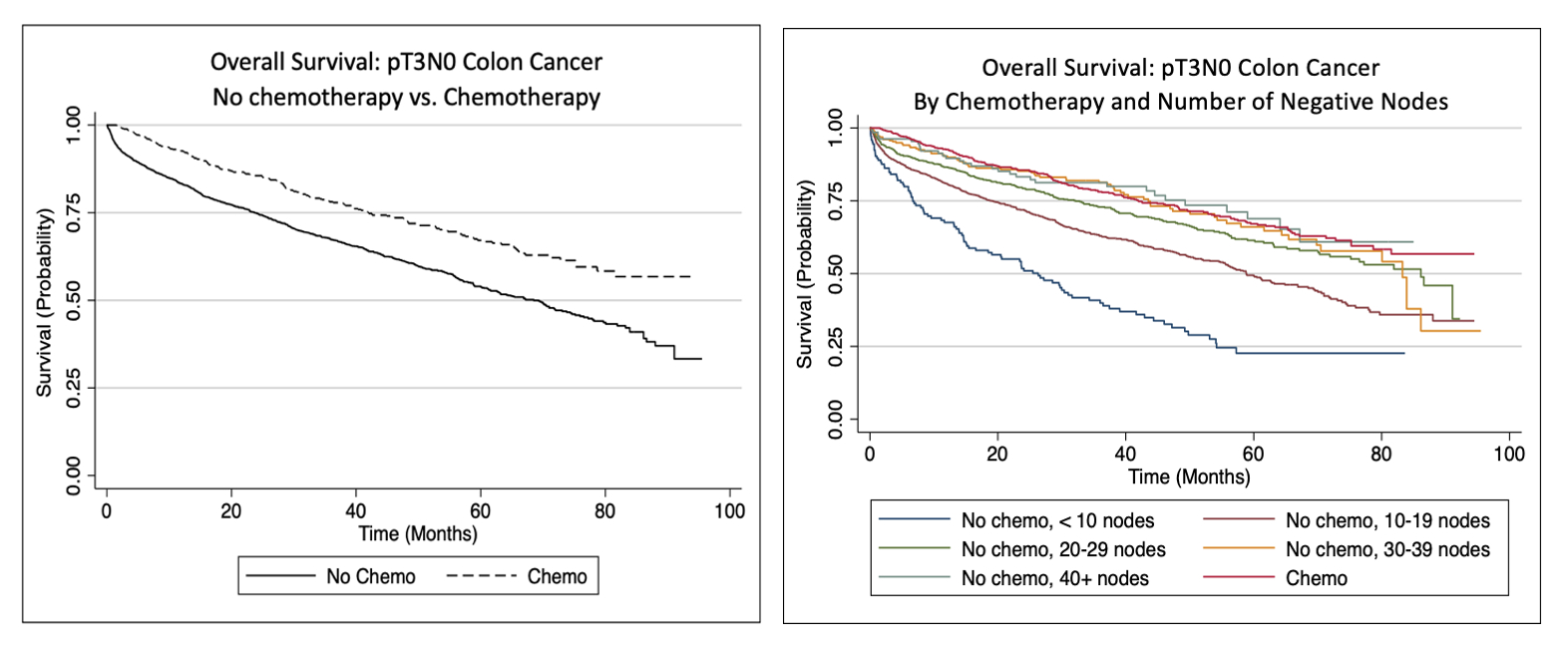
Results: There was a total of 3,645 patients identified. 2,839 (77.9%) patients received no chemotherapy while 806 (22.1%) patients received chemotherapy. Chemotherapy was associated with improved overall 5-year survival (HR 0.54, 95% CI: 0.5-0.6, p <0.001, Figure 1a). The 5-year overall survival for patients who received chemotherapy was 67%. In patients who did not receive chemotherapy with <10 nodes, 10-19 nodes, 20-29 nodes, 30-39 nodes, and 40+ nodes retrieved that were negative the 5-year overall survival was 22%, 49%, 61%, 66%, 69%, respectively (Figure 1b). When comparing patients with 30+ negative nodes who did not receive chemotherapy with patients who received chemotherapy, there was no significant difference in 1-year or 5-year overall survival (1-year survival 90% and 92%, respectively; 5-year survival 67% and 67%, respectively; p=0.56). In adjusted analysis, increasing age and higher Charlson Comorbidity Index were associated with significantly decreased overall survival while increasing number of negative lymph nodes was associated with significantly improved overall survival (all p<0.05).
Conclusions: Patients with T3N0 colon cancer with high-risk features who underwent adjuvant chemotherapy had improved overall survival. However, when stratified by lymph node harvest, patients who did not undergo chemotherapy who had <10 nodes or 10-19 nodes examined had the lowest overall survival and this was substantially different than for patients who received chemotherapy. On the other hand, there was no difference in overall survival between patients with 30+ nodes that were negative who did not receive chemotherapy when compared to patients undergoing chemotherapy. Decisions regarding adjuvant chemotherapy for patients with T3N0 colon cancer must be individualized and take into account lymph node harvest.
Back to 2022 Abstracts