
The impact of a multidisciplinary COVID-19 testing protocol on surgical volume: the Hartford Healthcare experience.
Bret Schipper, Oscar Serrano, Pavlos Papasavas, Mitch McClure, Ajay Kumar, jeffrey Cohen, Steven Shichman, Rekha Singh, william Sardella, Rocco Orlando
University of Connecticut, Farmington, CT, United States Minor Outlying Islands
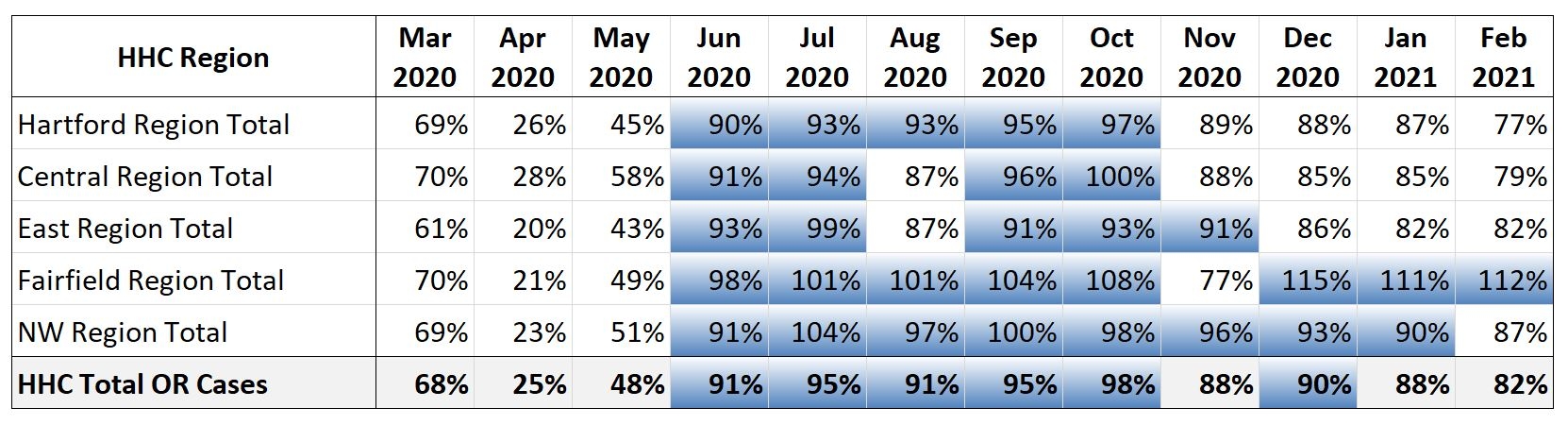
Objective The initial wave of the COVID-19 pandemic compelled hospitals to reduce surgery and procedure volumes to preserve resources. Surgery resumption was critical to providing necessary care that had been deferred while preserving capacity for managing COVID-19. The study objective is to show that through our robust testing model as well as by using lessons learned from the first wave and a comprehensive COVID management strategy, we could maintain an increasing volume of surgery during the second and third COVID-19 phase. Design Retrospective pre-/post-interventional observational study Setting 7-hospital (2,427 in-patient beds, 26,647 in-patient surgeries) healthcare system Patients (or Other Participants) Patients in need of surgery within our healthcare system. Interventions A multidisciplinary Pivot Plan was implemented to safely allow patients needing surgical care to receive treatment. This plan incorporated changes such as changes in the electronic medical record, altered perioperative staff utilization, partnership with primary care, and use of a COVID-19 testing algorithm based on a pre-determined hierarchy of case acuity. The Pivot Plan was also intended to mitigate the impact of increasing COVID numbers. We evaluated the change in surgery volume during the first, second, and third COVID-19 phases (Phase 1: Mar2020-May 2020, Phase 2: June 2020-Oct 2020, Phase 3:Nov 2020-Feb 2021) Main Outcome Measure (s)
Surgery volumes at all Hartford Healthcare facilities FY 2020 through FY 2021 (February) Results The Pivot Plan was studied from March 2020 to February 2021. During the first phase, 8125 patients were tested for COVID-19 in anticipation of surgery; 35 (0.4%) tested positive for COVID-19 and had their procedure deferred. As testing capability increased, we were able to increase our added surgery capacity from 13 cases per day to 531 cases per day. In turn, we saw the case volume increase by 47% after the first wave. We compared Phase 1,2, and 3 time period volumes to their historical volumes one year earlier at the same time intervals. During wave one, we performed 47% fewer cases than the historical average. During the second phase, when positivity levels dropped again, we increased to 94% of the historical average. Finally, during phase 3 we when positivity rates spiked again, we were still able to maintain 87% of historical baseline averages Conclusions Although our health care system decreased all surgery during the first wave of COVID-19, Our ability to utilize pre-op testing, as well as a pivot utilizing comprehensive COVID management protocols, enabled us to safely pivot to restart surgery and increase volume during the second wave while still delivering safe care to our patients.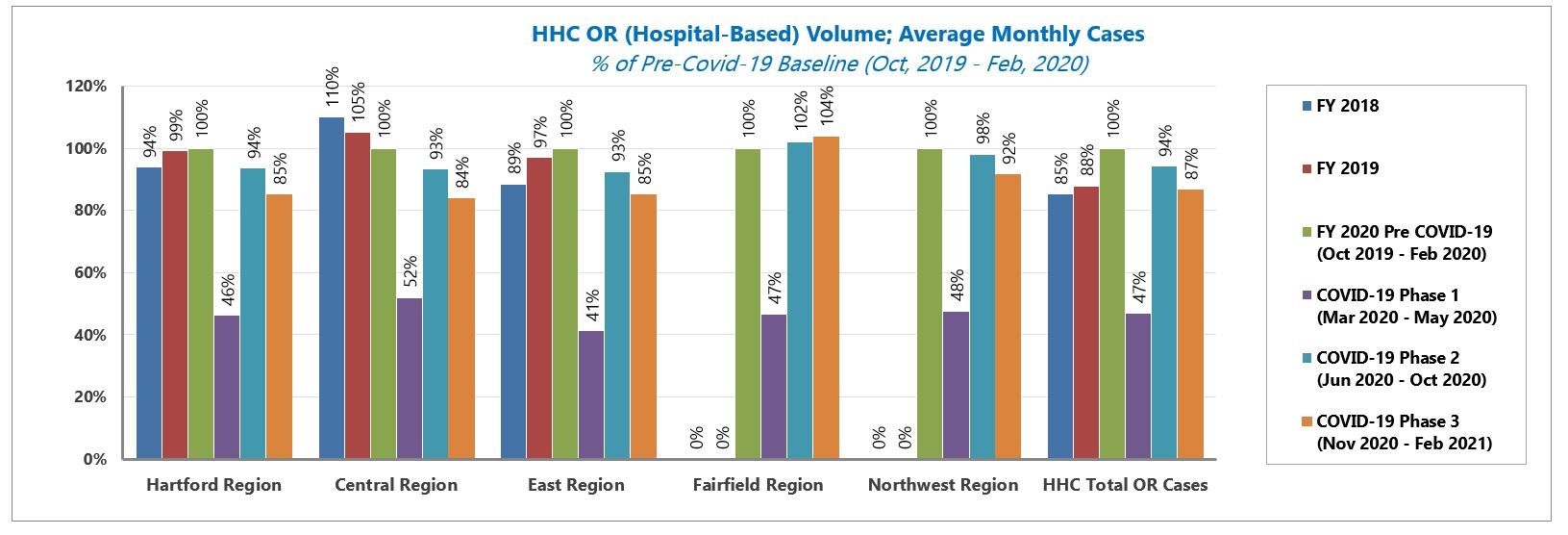

Back to 2021 Posters