
Hospital-Based Variations in Geriatric Surgical Safety for Emergency Operations
*Robert D Becher, *Michael P DeWane, *Nitin Sukumar, *Marilyn J. Stolar, *Thomas M. Gill, *Cheryl K. Zogg, Kevin M. Schuster, Adrian A. Maung, Kimberly A. Davis
Yale School of Medicine, New Haven, CT
Objective: To quantify the variations in hospital standardized mortality associated with emergency operations in geriatric patients, and determine whether the differences can be explained by patient- and hospital-level characteristics among outlier-hospitals.
Design: Retrospective cohort study.
Setting: Acute care hospitals.
Patients: 65-years-and-older who underwent one of eight common emergency general surgery (EGS) operations identified using the California Inpatient Database (2010-2011).
Main Outcome Measures: Risk-adjusted hospital-level standardized mortality ratio (SMR; ratio of observed-to-expected in-hospital deaths; average SMR=1.0). High-SMR (>1.0) and low-SMR (<1.0) outlier-hospitals (80% confidence interval not crossing SMR=1.0) were compared.
Results: 24,207 patients were included from 107 hospitals. SMR (Figure) varied widely, from 2.3 (highest) to 0.3 (lowest). 11 hospitals (10.3%) were poor-performing high-SMR-outliers, while 10 hospitals (9.3%) were exceptional-performing low-SMR-outliers. SMR was 3-times worse in the high-SMR compared to the low-SMR-outlier group (1.7 vs 0.6; p<0.001); the average number of EGS operations per institution in the two outlier groups was not significantly different (208 vs 261, respectively). Patient-level (age; gender; van-Walraven-comorbidity-score) and hospital-level (trauma center status; high-tech hospitals; teaching hospitals; hospital size >100 beds; rural location) characteristics were equivalent among outlier-hospitals. 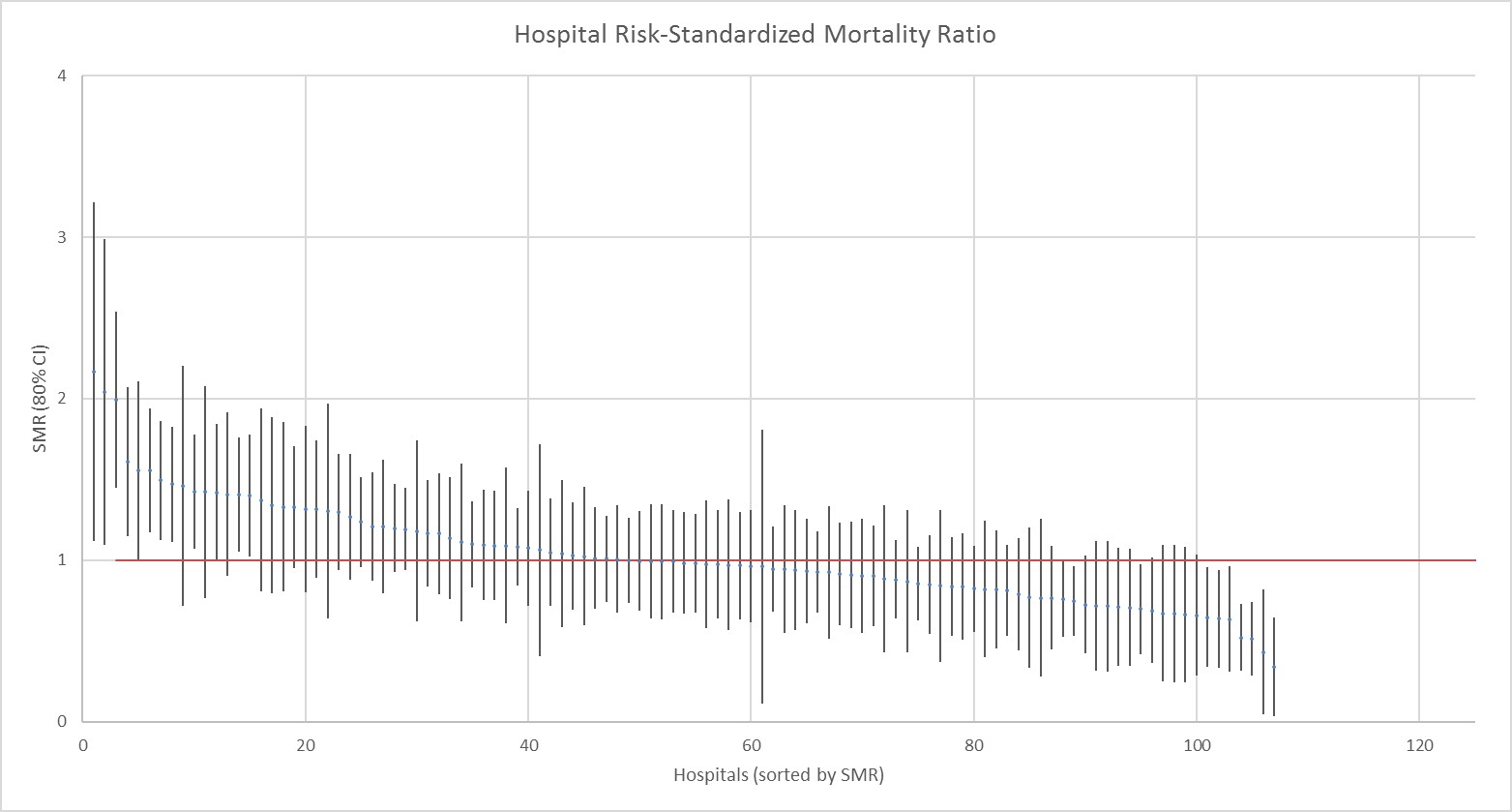
Conclusions: Significant hospital variation exists in standardized mortality after common general surgery operations done emergently in older patients. At over 10% of institutions there is substantial excess-mortality. The patient- and hospital-level characteristics studied do not explain the EGS survival-differential across institutions. These findings confirm that more work needs to be done to optimally integrate emergency surgery services across institutions to deliver high-value, low-mortality care to every geriatric surgical patient.
Back to 2019 Posters



