
Surgical Stabilization of Rib Fractures: A Single Institution's Experience
*Erica D Kane, *Elan Jeremitsky, *Susan Kartiko, Andrew R Doben
Baystate Medical Center, Springfield, MA
Objective: Utilization of surgical stabilization for rib fractures (SSRF) has increased. Despite compelling small studies, many centers still struggle in determining criteria for intervention. We analyzed our patient outcomes compared to non-operative (NonOp) National Trauma Databank (NTDB) Controls. Design: Retrospective comparison of SSRF versus NonOp controls from the NTDB. Setting: Level I trauma center.
Patients: Trauma patients with ≥5 rib fractures and flail diagnosis (ICD 807.4 and AIS predot codes) Intervention: SSRF versus NonOp Main Outcome Measures: Mortality, pneumonia, Length of Stay (LOS), ICU LOS, ventilator use, tracheostomy rates. Results: Overall, SSRF patients were older, had worse respiratory comorbidities and similar injury severity scores (ISS) (Table1). Despite more respiratory disease in SSRF patients versus NonOp (p<0.0001), ventilator use was lower for SSRF (p=0.006), as was ICU LOS (p=0.025). SSRF resulted in decreases in mortality (12.8%, p<0.0001) and pneumonia (12.1%, p=0.008) compared to NonOp on propensity score matching. On subgroup analysis of patients ≥65 years of age, ISS remained similar between groups (Table1). Mortality remained improved for SSRF versus NonOp (p=0.02) even with worse respiratory disease (p<0.0001). Conclusion: Patients who underwent SSRF at our institution had improved outcomes despite worse respiratory comorbidity compared to patients who were managed non-operatively nation-wide. Mortality remained improved for age ≥65 suggesting age should not be restrictive of intervention. 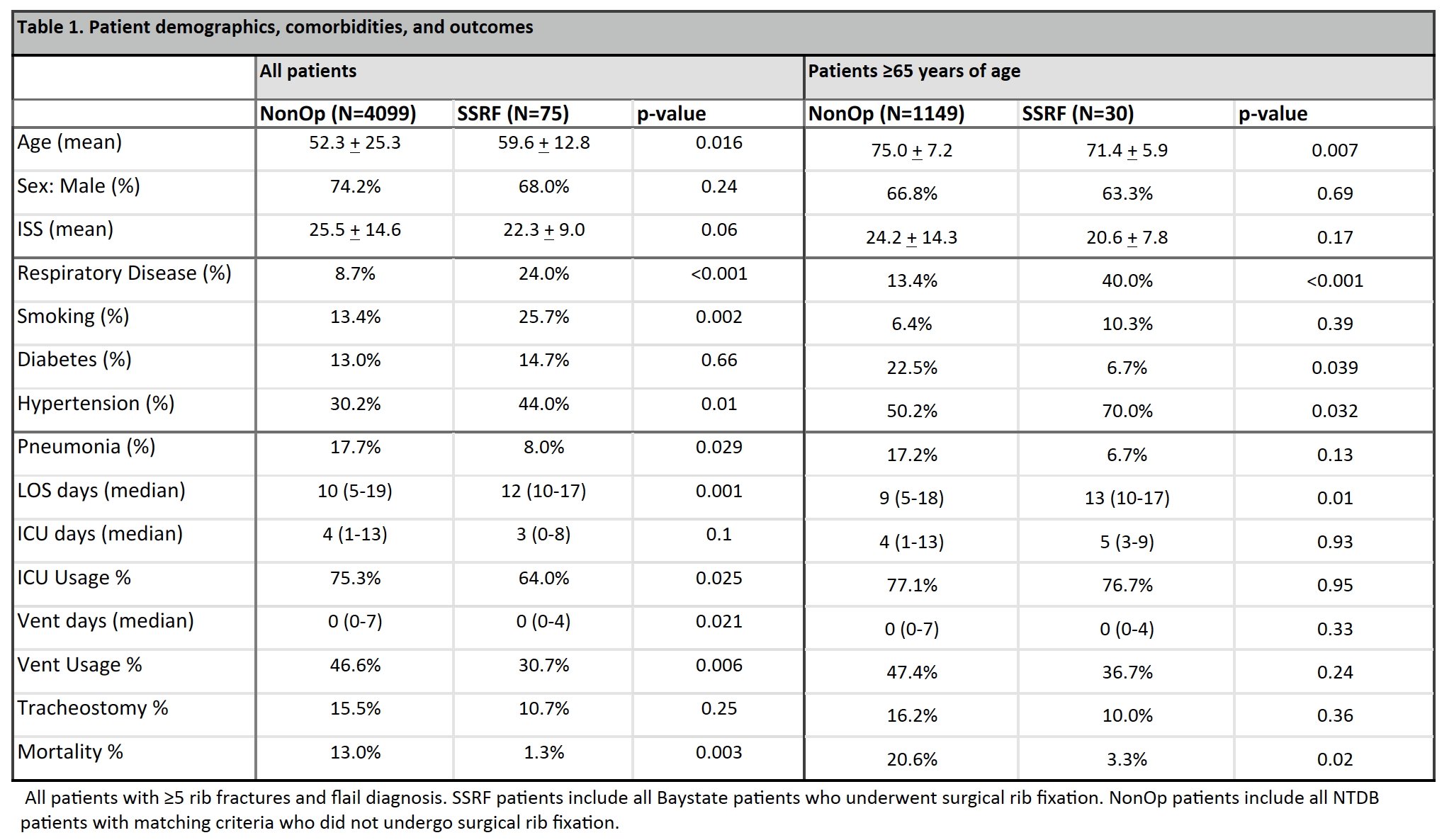
Back to 2017 Program