| Current Meeting Home | Final Program | Past & Future Meetings |
|
Back to 2016 Annual Meeting Posters Outcomes and Effects of an Advanced Endoscopy Center and GI Center of Excellence on Pancreatic Cancer Surgical Volume *Rachel E Beard, *Mariam F Eskander, *Gyulnara Kasumova, *Abhishek Tadikonda, *Tyler M Berzin, *Mandeep Sawhney, *Ram Chuttani, *Douglas K Pleskow, Mark P Callery, Jennifer F Tseng Beth Israel Deaconess Medical Center, Boston, MA
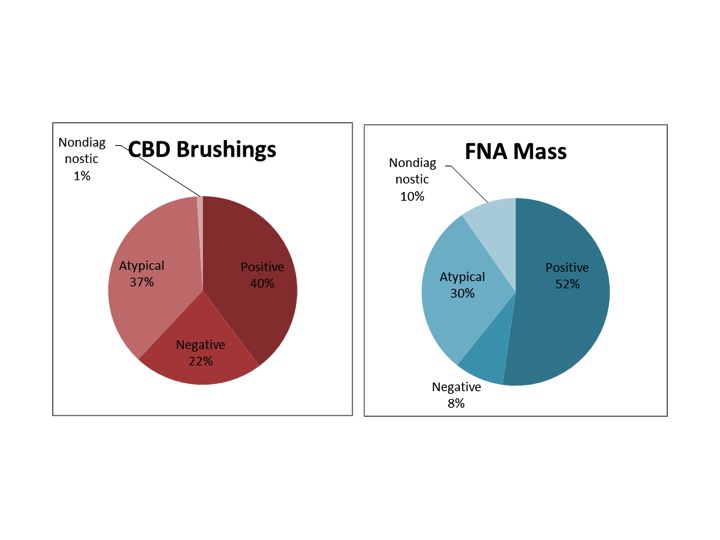
Objective: The safety and utility of advanced endoscopic procedures in the diagnosis and management of pancreatic cancer were investigated. Design: A retrospective, single-institution contemporary cohort study. Setting: A high-volume pancreatic cancer center and GI center of excellence. Patients: Patients with pancreatic cancer diagnosed 2006-2012 at our institution. Interventions: All patients had at least one cancer-related ERCP. Stents, brushings and other endoscopic procedures were documented. Main Outcome Measures: 30-day complications, diagnostic sensitivity, and time to treatment. Results: 503/968 (52.0%) of all pancreatic cancer patients had an in-house ERCP. 388 (77.1%) underwent endobiliary stenting at first ERCP (258 plastic, 130 metal), and 298 (59.3%) had common bile duct (CBD) brushings (diagnostic sensitivity=54%). 37 (7.4%) experienced a 30-day complication. 210 (41.8%) received a second ERCP in a median time of 42 days (IQR 11, 33). 254 (50.5%) also received endoscopic ultrasound (EUS), 176 of whom had fine needle aspiration (FNA) of a mass (sensitivity=77%). 242 (48.1%) first obtained a definitive diagnosis via endoscopy: 15 in 2006 vs. 59 in 2012 (p<0.0001). Of 236 resected patients, 52.5% required an ERCP; median time to resection from prior ERCP was 18 days (IQR 11,31). In unresected patients who had ERCP before documented chemotherapy (n=143), median time to chemotherapy was 41 days (IQR 22, 65). Conclusions: Endoscopy is increasingly employed in the diagnosis and management of pancreatic cancer patients. Understanding its advantages and limitations is valuable for surgeons in a multidisciplinary environment. Careful communication can optimize decisions regarding stents, diagnostic procedures, and timing of treatment. Back to 2016 Annual Meeting Posters |
|
| © 2026 New England Surgical Society. All Rights Reserved. Privacy Policy. |