|
Back to Annual Meeting Program
Improving Operating Room Turnover
*Ankeet S. Bhatt1, *Grant W. Carlson2, Peter J. Deckers1
1University of Connecticut School of Medicine, Farmington, CT;2Emory University School of Medicine, Atlanta, GA
Objective: Develop a system-based turnover redesign to reduce turnover time (TT).
Design: Prospective case analysis.
Setting: 511 bed academic medical center (AMC) - 24 operating rooms.
Patient/Other Participants: Turnover redesign compared against two controls:
1. 237 turnovers (all specialties).
2. 13 observations (Vascular and Orthopedics).
Inclusion criteria: case-to-follow TT. Exclusion criteria: add-on and/or emergent cases.
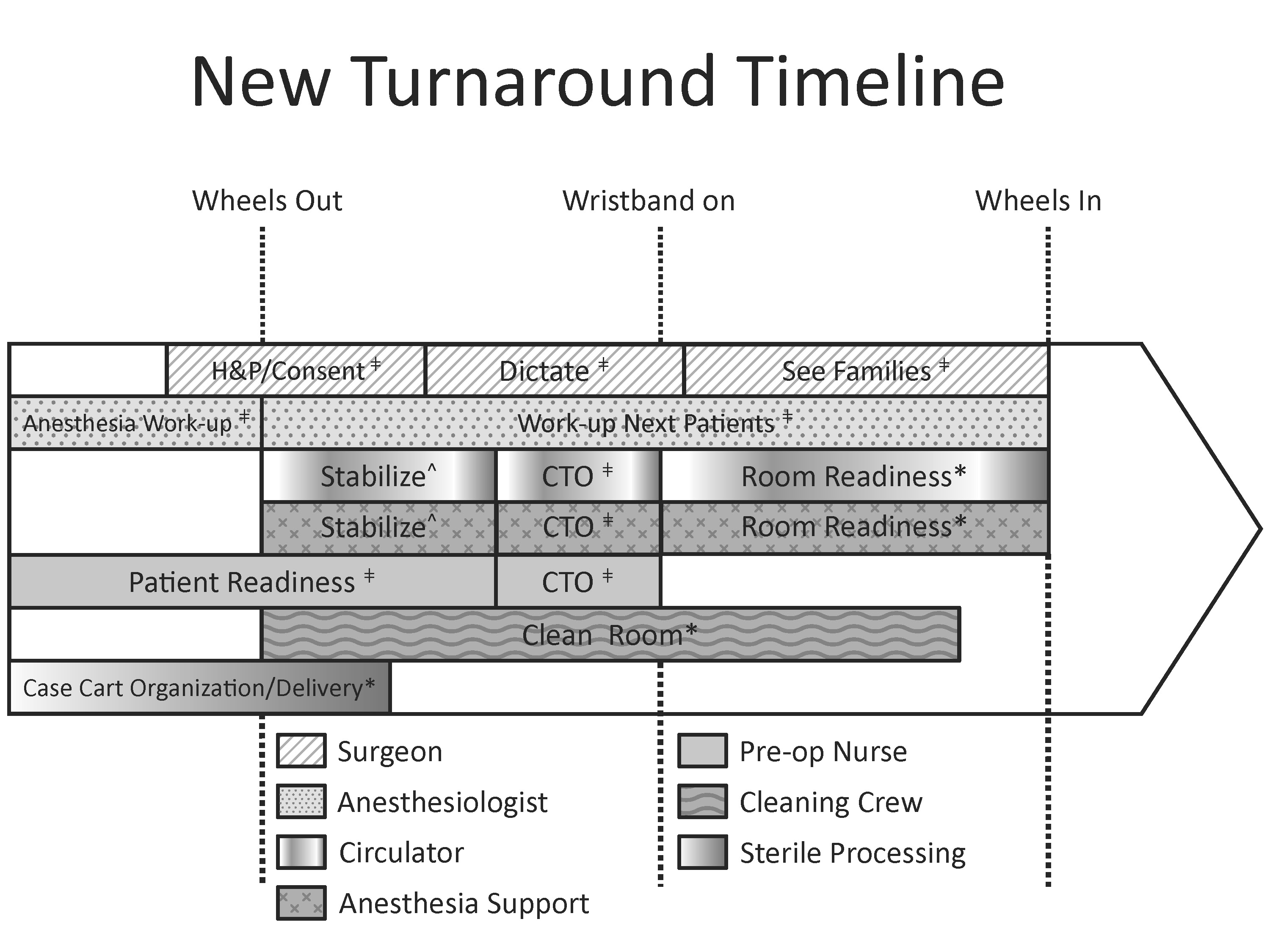
Intervention: Three major interventions were undertaken: developing a consistent criteria for OR readiness, utilizing parallel processing for patient and room readiness, and enhancing perioperative communication. Process redesign implemented in Vascular and Orthopedics.
Turnover Redesign (see Image)
ǂ Pre-op Holding Area.
CTO: Call to Order – Final Perioperative Check
* Operating Room.
^ Post-Anesthesia Care Unit (PACU).
Main Outcome Measures: Mean TT (wheels in to wheels out) and standard deviation of TT. Secondary outcome measure: frequency of TT ≥ 30 minutes.
Results: Using all specialty controls, mean TT (h:mm:ss) was reduced by 0:20:48 minutes (95% CI, 0:10:46-0:30:50); standard deviation by 0:10:32 minutes, from 0:16:24 to 0:05:52; frequency of TT≥ 30 minutes from 72.5% to 11.7%.
Using Vascular and Orthopedics controls, mean TT was reduced by 0:15:16 minutes (95% CI, 0:07:18-0:23:14); standard deviation from 0:14:39 to 0:05:52; frequency of TT≥ 30 minutes from 69.2% to 11.7%. P<0.001 for all reductions.
Conclusion: Reductions in mean TT present major efficiency, patient care, and financial opportunities. Historical data shows 10-19 minute reductions in mean TT reduce staffing costs 2.5- 4.0%, representing yearly savings of $626,100 at a similarly matched AMC. A systems-based focus should drive OR turnover design.
Back to Annual Meeting Program
|
|
